Original article
Beyond access: mental health among racialized Brazilian women in Portugal / Más allá del acceso: mujeres brasileñas racializadas y salud mental en Portugal / Para além do acesso: mulheres brasileiras racializadas e saúde mental em Portugal
Izabela Pinheiro1 (https://orcid.org/0000-0003-0189-7967)
Mariana Holanda Rusu2 (https://orcid.org/0009-0000-3994-8315)
Conceição Nogueira3 (https://orcid.org/0000-0002-9152-754X)
Joana Topa4 (https://orcid.org/0000-0003-0663-973X)
1Corresponding contact. Universidade do Porto (Porto). Portugal. [email protected]
2-3Centro de Psicologia da Universidade do Porto, Universidade do Porto (Porto). Portugal. [email protected], [email protected]
4Universidade da Maia (Maia). Portugal. [email protected]
ABSTRACT | INTRODUCTION: The migratory flow of Brazilian women to Portugal has intensified in recent decades, driven by expectations of security, stability, and better living conditions. However, lived reality often contrasts sharply with these expectations, marked by precarious employment, institutional racism, and social exclusion, factors that generate psychological distress and motivate the search for psychological support. OBJECTIVE: To understand how racialized Brazilian women experience seeking and receiving psychological support in Portugal, considering the social markers of difference, gender, race, class, and nationality. METHOD: This qualitative study, grounded in intersectional and decolonial feminism and social constructionism, conducted fifteen semi-structured interviews with immigrant women who sought psychological care after migration. Data were analyzed using reflexive thematic analysis. RESULTS: The analysis revealed that the search for care emerges as a response to structural suffering, caused by the gap between expectations of welcome and experiences of discrimination, loneliness, and instability. Participants faced multiple access barriers, financial, bureaucratic, and symbolic, that evidence the persistence of colonial hierarchies in mental health services. In the therapeutic setting, the absence of multicultural competencies resulted in experiences of silencing, misunderstanding, and revictimization. As a counterpoint, creative resistance strategies emerged, such as online therapy with Brazilian professionals and engagement with community-based care networks. CONCLUSION: The study contributes to contemporary debates on migration, mental health, and intersectionality, reinforcing the urgency of culturally responsive public policies and clinical practices committed to social justice, ethics of care, and the decolonization of psychology.
KEYWORDS: Psychological Stress. Racism. Cultural Competency. Social Discrimination. Psychotherapy.
RESUMEN | INTRODUCCIÓN: El flujo migratorio de mujeres brasileñas hacia Portugal se ha intensificado en las últimas décadas, impulsado por expectativas de seguridad, estabilidad y mejores condiciones de vida. Sin embargo, la realidad vivida a menudo contrasta con estas expectativas, marcada por la precarización laboral, el racismo institucional y la exclusión social, factores que generan malestar psicológico y motivan la búsqueda de apoyo psicológico. OBJETIVO: Comprender cómo las mujeres brasileñas racializadas experimentan la búsqueda y recepción de apoyo psicológico en Portugal, considerando los marcadores sociales de la diferencia, como género, raza, clase y nacionalidad. MÉTODO: Este estudio cualitativo, fundamentado en el feminismo interseccional y decolonial y en el construccionismo social, realizó quince entrevistas semiestructuradas con mujeres inmigrantes que buscaron atención psicológica después de la migración. Los datos se analizaron mediante análisis temático reflexivo. RESULTADOS: El análisis reveló que la búsqueda de atención emerge como respuesta a un sufrimiento estructural, causado por la brecha entre las expectativas de acogida y las experiencias de discriminación, soledad e inestabilidad. Las participantes enfrentaron múltiples barreras de acceso financieras, burocráticas y simbólicas, que evidencian la persistencia de jerarquías coloniales en los servicios de salud mental. En el encuadre terapéutico, la ausencia de competencias multiculturales resultó en experiencias de silenciamiento, incomprensión y revictimización. Como contrapunto, emergieron estrategias creativas de resistencia, como la atención online con profesionales brasileños/as y la articulación con redes comunitarias de cuidado. CONCLUSIÓN: El estudio contribuye a los debates contemporáneos sobre migración, salud mental e interseccionalidad, reforzando la urgencia de políticas públicas y prácticas clínicas culturalmente responsivas, comprometidas con la justicia social, la ética del cuidado y la descolonización de la psicología.
PALABRAS CLAVE: Estrés Psicológico. Racismo. Competencia Cultural. Discriminación Social. Psicoterapia.
RESUMO | INTRODUÇÃO: O fluxo migratório de mulheres brasileiras para Portugal tem se intensificado nas últimas décadas, impulsionado por expectativas de segurança, estabilidade e melhores condições de vida. No entanto, a realidade vivida muitas vezes contrasta com essas expectativas, sendo marcada por precarização laboral, racismo institucional e exclusão social, fatores que geram sofrimento psíquico e motivam a busca por apoio psicológico. OBJETIVO: Compreender como mulheres brasileiras racializadas experienciam a busca e o recebimento de apoio psicológico em Portugal, considerando os marcadores sociais da diferença, como gênero, raça, classe e nacionalidade. MÉTODO: Este estudo qualitativo, fundamentado no feminismo interseccional e decolonial e no construcionismo social, realizou quinze entrevistas semiestruturadas com mulheres imigrantes que buscaram acompanhamento psicológico após a migração. Os dados foram analisados através de análise temática reflexiva. RESULTADOS: A análise revelou que a busca por cuidado emerge como resposta a um sofrimento estrutural, provocado pelo descompasso entre expectativas de acolhimento e vivências de discriminação, solidão e instabilidade. As participantes enfrentaram múltiplas barreiras de acesso financeiras, burocráticas e simbólicas, que evidenciam a permanência de hierarquias coloniais nos serviços de saúde mental. No contexto terapêutico, a ausência de competências multiculturais resultou em experiências de silenciamento, incompreensão e revitimização. Como contraponto, emergem estratégias criativas de resistência, como o atendimento online com profissionais brasileiras/os e a articulação com redes comunitárias de cuidado. CONCLUSÃO: O estudo contribui para os debates contemporâneos sobre migração, saúde mental e interseccionalidade, reforçando a urgência de políticas públicas e práticas clínicas culturalmente responsivas, comprometidas com a justiça social, a ética do cuidado e a descolonização da psicologia.
Palavras-chave: Estresse Psicológico. Racismo. Competência Cultural. Discriminação Social. Psicoterapia.
How to cite this article: Pinheiro, I., Rusu, M. H., Nogueira, C., & Topa, J. (2026). Beyond access: mental health among racialized Brazilian women in Portugal. Revista Psicologia, Diversidade e Saúde, 15, e6637. https://doi.org/10.17267/2317-3394rpds.2026.e6637
Submitted Dec. 9, 2025, Accepted Apr. 14, 2026, Published June 12, 2026
Rev. Psicol. Divers. Saúde, Salvador, 2026;15:e6637
https://doi.org/10.17267/2317-3394rpds.2026.e6637
ISSN: 2317-3394
Assigned editors: Mônica Daltro, Marilda Castelar, Martha Castro
Short title: Mental health among racialized Brazilian women in Portugal
Título corto: Mujeres brasileñas racializadas y salud mental en Portugal
Título curto: Mulheres brasileiras racializadas e saúde mental em Portugal
Introduction
Women's migration from the Global South to the Global North is marked by expectations of better living conditions, security, and stability. However, the gap between imagined opportunities and lived realities is often profound, with many facing precarious employment and institutional challenges (Azevedo et al., 2022). Many immigrants face precarious labor conditions and economic vulnerability, which contribute to psychological distress (Alarcão et al., 2024). In Portugal, this context is compounded by rising anti-migrant discourse and growing far-right influence, which fuel exclusionary narratives (Stevens et al., 2024).
This gap between expectation and reality generates persistent insecurity, fear, and invisibility, leading to profound psychological distress. This suffering constitutes structural violence produced by systems that hierarchize lives, shaped by intersecting inequalities (Collins & Bilge, 2021; Crenshaw, 2017), and compounded by barriers to accessing healthcare (Tourinho et al., 2024). Such distress is not experienced homogeneously; the intersections of gender, race, class, and nationality shape specific vulnerabilities and influence migration trajectories (Collins & Bilge, 2021; Crenshaw, 2017). Migration's ambivalent nature exposes women to new forms of structural violence while potentially serving as a path toward emancipation and identity reconstruction (Azevedo et al., 2022; Lantz et al., 2023).
Racialization is understood as a social and historical process of hierarchizing bodies and identities, operating through the ascription of unequal meanings to accents, nationalities, and cultural practices (Kilomba, 2019; Vergès, 2020). From a decolonial perspective, all Brazilian women are subject to racialization processes in Portugal, positioned as "others" existing outside normative standards. However, skin color intersects with other markers, such as accent, nationality, gender, and class, to produce differentiated intensities and forms of exclusion. This requires a reflection on whiteness and non-whiteness and the construction of normative models of mental health (Pereira, 2022). This conceptual choice is deliberate, moving beyond the fixed categories often used in public health to focus on racism as a dynamic process that produces social inequalities, a perspective that is central to the decolonial and intersectional framework of this study.
The shared language and historical ties between Brazil and Portugal, while often framed as facilitating integration, can reinforce subtle forms of racism disguised as familiarity, operating through disqualification and objectification (França & Oliveira, 2021). These mechanisms permeate migrants’ daily lives and restrict their access to rights and dignified living conditions. Psychological distress thus emerges as an expression of exclusion and intersectional violence, revealing the persistence of colonial boundaries inscribed on these women's bodies and lives (Barata, 2022).
Faced with these conditions, many migrant women seek psychological support as a strategy for survival and resistance, typically in moments of crisis triggered by discrimination, social isolation, and migration-related stressors (Alarcão et al., 2024; Ryan et al., 2021; Teixeira et al., 2025). Research indicates that immigrants, especially women, are more vulnerable to developing depression, anxiety, post-traumatic stress, and suicidal ideation than native populations (World Health Organization [WHO], 2025).
Psychosocial impacts are directly linked to living conditions and structural exclusion, which are often medicalized rather than addressed as social determinants of health (Lantz et al., 2023). Seeking psychological help thus extends beyond the individual realm and assumes a political dimension, asserting the right to exist with dignity, particularly for women facing gender-based vulnerabilities (Tourinho et al., 2024).
However, access to culturally sensitive psychological care remains limited. In Portugal, migrant women face long waiting lists, excessive bureaucracy, and high costs for private services (Inácio et al. 2025). These barriers are compounded by subtler forms of exclusion grounded in colonial hierarchies and universalist conceptions of clinical care that disregard social and cultural differences (Pussetti et al., 2009). Despite the rhetoric of the universality of the National Health Service (SNS), significant asymmetries persist, including linguistic and cultural barriers, institutional distrust, a scarcity of interculturally trained professionals, and the absence of protocols guiding culturally responsive practices (Inácio et al., 2025; Tourinho et al., 2024). For migrants with irregular status, these barriers are even more severe, often resulting in the denial of basic rights and discouragement from seeking support (Stevens et al., 2024). Similar dynamics have been observed in Canada, where racialized immigrants face persistent inequalities in access to and quality of mental healthcare, highlighting the structural limits of systems that, although universal, reproduce racial hierarchies (Lin, 2023).
Between invisibility and insurgency: racialized Brazilian women and psychological support in Portugal
Among those who access psychological services, many report encountering psychologists who struggle to understand the specificities of migration experiences and how gender, class, race, and nationality intersect to shape migrants' psychological distress. Lack of cultural competence manifests in minimizing racism and xenophobia incidents, individualizing socially produced suffering, and reproducing stereotypes within therapeutic encounters (Pussetti et al., 2009). Spaces intended for listening and support can thus become sites of revictimization, where suffering is reduced to individual symptoms detached from the social causes. Similar phenomena have been observed in other European countries, where the absence of empathetic spaces limits migrant patient engagement (Radl-Karimi et al., 2022). These gaps highlight the limitations of mental health systems in addressing colonial and intersectional power dynamics (Pereira, 2022).
In response, migrant women have developed alternative strategies for accessing psychological care that transcend national borders and challenge the institutional logic. Seeking therapists of the same nationality, whether residing in Brazil or abroad, offering online support, has consolidated as a transnational practice of resistance, motivated by the need for safe and validating spaces. Sharing a common symbolic world eliminates the need to translate or justify experiences, allowing for immediate and deep therapeutic connections (Pussetti et al., 2009). Sharing language and cultural references is central to building trust and facilitating emotional expression, particularly for Brazilian migrant women seeking validation through online sessions with their compatriots (Teixeira et al., 2025).
Technology-based interventions have been associated with reductions in psychological distress among immigrant and refugee populations (Hynie et al., 2023), and cultural and linguistic proximity has been identified as a factor that facilitates therapeutic engagement and improves service utilization (Lin, 2023).
These practices are mediated by informal immigrant support networks, where recommendations and experiences are shared, and care repertoires are collectively constructed. Alongside individual psychotherapy, immigrant collectives and peer support groups function as significant care arrangements for these populations (Teixeira et al., 2025). Such practices address gaps in Portuguese services and represent forms of agency that challenge Eurocentric therapeutic epistemologies. By creating transnational and community-based support circuits, women develop alternative care pathways grounded in shared validation and the rejection of practices that render them invisible or pathologize their experiences (Pussetti et al., 2009; Pereira, 2022).
While the international literature on migrant mental health has expanded, most studies have focused on service access, prevalence of disorders, and structural barriers (WHO, 2025). Few studies have examined the quality of the therapeutic relationship and migrants' lived experiences during psychological care (Pussetti et al., 2009; Radl-Karimi et al., 2022). Even rarer are studies incorporating intersectional and decolonial perspectives to explore how gender, race, class, and nationality shape the possibilities for listening and clinical care (Rocha-Jiménez et al., 2025). In the Portuguese context, despite the significant growth of Brazilian migration and women's central role, research remains scarce on the experiences of seeking and receiving psychological support and on the transnational and collective strategies developed to overcome system limitations.
Based on this scenario, the present study investigates, from an intersectional feminist and decolonial epistemology, the following research question: How do racialized Brazilian women experience access to and engagement with psychological support in Portugal, and how are these experiences shaped by the intersecting dynamics of gender, race, socio-economic class, and nationality? Guided by this question, this study seeks to understand how these women construct meaning around their experiences of accessing and engaging with psychological support, analyzing how structural inequalities are reflected in therapeutic relationships and shape care opportunities. This study also aims to identify individual, collective, and transnational strategies developed to overcome the limitations of the Portuguese psychological support system, thereby expanding the available care repertoire. This research contributes to the development of culturally responsive and structurally competent psychological practices aligned with commitments to equity, social justice, and the recognition of Global South women's epistemologies and experiences in mobility contexts.
Method
This qualitative, exploratory study is guided by a framework integrating intersectional and decolonial feminism (Collins & Bilge, 2021; Crenshaw, 2017; Vergès, 2020) and social constructionism (Rogers & Willig, 2017). This lens allows for understanding the pursuit of psychological support as an experience situated at the intersections of gender, race, class, and nationality, recognizing that suffering and care are produced within historical and political contexts that shape who receives therapeutic support. Reporting followed the recommendations of the Consolidated Criteria for Reporting Qualitative Research (COREQ), which provide guidance for ensuring transparency and rigor in qualitative research reporting (Tong et al., 2007).
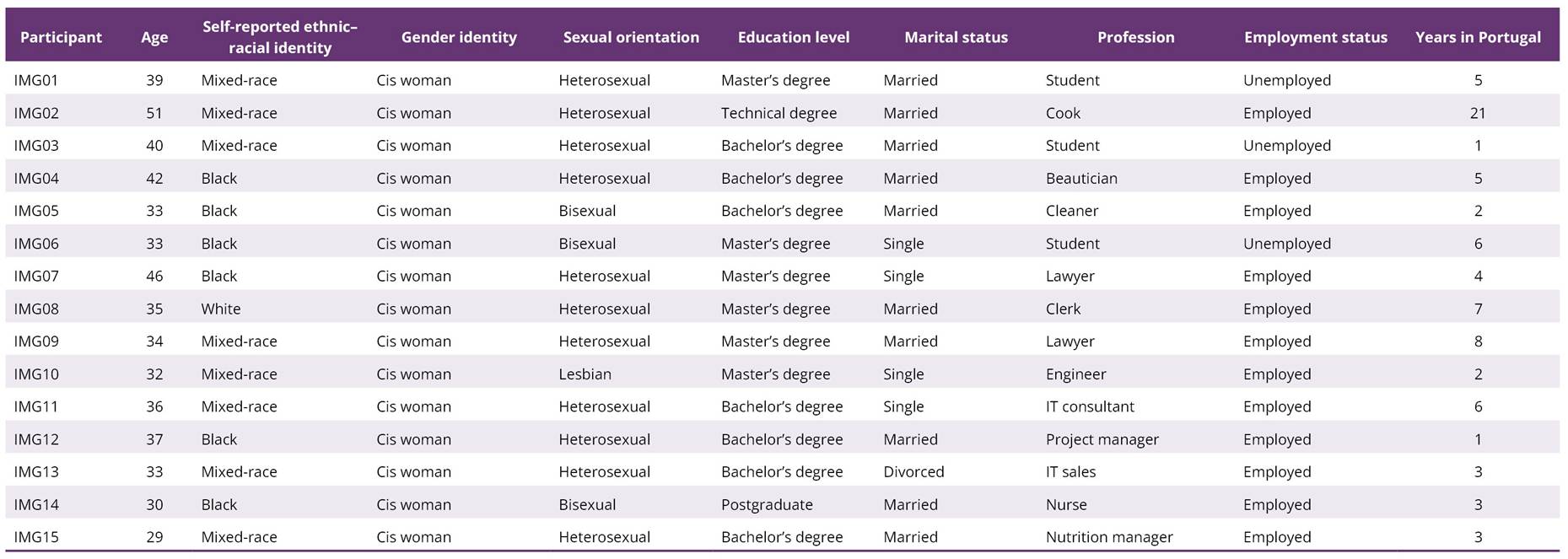
Fifteen Brazilian women residing in Portugal participated, meeting the criteria of: (a) being a Brazilian woman living in Portugal; (b) being 18 years or older; and (c) having sought psychological support after migration. Ages ranged from 29 to 51 years (M = 37.1; SD = 6.4). Six participants identified as Black, eight as mixed-race, and one as White. While all participants, as Brazilian women in Portugal, are subject to racialization processes, skin color was documented to capture the intersectional diversity of experiences, recognizing that racialization operates with differentiated intensities and forms. All were cisgender women. Education levels ranged from a technical degree to a master's degree. Twelve participants were employed, and three were students. Length of residence in Portugal varied from one to twenty-one years (M = 5.1; SD = 4.9). The number of participants was considered appropriate to generate rich and meaningful interpretations, consistent with the epistemological assumptions of Reflexive Thematic Analysis, which prioritizes depth of engagement with the data rather than the achievement of data saturation (Braun & Clarke, 2021). A summary of sociodemographic characteristics is provided in Table 1.
Table 1.
Socio-demographic characteristics of the participants
Data were collected through individual semi-structured interviews conducted between May and October 2024, with an average duration of 90 minutes. Interviews were conducted online and followed a guide composed of two parts. All interviews were conducted by the first author, a psychologist and doctoral researcher with prior experience in qualitative studies on migration and mental health. Sharing language and cultural background with participants facilitated rapport during the interviews, while reflexive attention was maintained regarding potential power asymmetries and the influence of the researcher’s positionality on the research process. The first part of the interviews included questions developed based on a literature review on migration, mental health, and culturally responsive psychological practices, organized into two main thematic axes:
1) Psychological support: addressing motivation to seek help, the process of accessing services, and experiences in psychotherapy, including perceptions of professionals’ technical and personal preparation, challenges and achievements within the therapeutic relationship, and the psychosocial impacts of support received (e.g., “What motivated you to seek psychological support after migration?”, “How did you find and access this service?”, “Did psychological support significantly impact your life?”);
2) Multicultural competencies and recommendations: exploring participants’ perceptions of psychologists’ work with racialized migrant populations, as well as suggestions for improving clinical practices (e.g., “As a racialized immigrant woman, what recommendations would you offer to psychology professionals working with this population?”).
The second part of the guide consisted of a sociodemographic questionnaire aimed at characterizing participants’ profiles, including variables such as age, length of residence in Portugal, education, marital status, professional area, and employment status.
To ensure that the instrument accurately reflected the study objectives, the Vali-Quali qualitative validation framework was applied, enabling evaluation of the content and semantics of semi-structured interview guides. The process involved six integrated steps: drafting, expert review, analysis of results, pretesting, refinement, and validation, culminating in the final theoretical–empirical version of the instrument. Validity was assessed according to four dimensions: coherence with research objectives, alignment with theoretical constructs, clarity of language, and adequacy for qualitative inquiry (Torlig et al., 2022). Two experts (PhDs in Social Psychology) reviewed the guide for clarity, relevance, and coherence, and their feedback was incorporated. This process strengthened the study’s methodological rigor by ensuring that the instrument was consistent with the research objectives and theoretical framework.
Participants were recruited using convenience and snowball sampling through social media and partnerships with immigrant collectives. Initial contact occurred via email or phone, during which study objectives and ethical procedures were explained. No refusals were recorded among those who were contacted and met the eligibility criteria. Participation was voluntary and formalized through a signed informed consent form, which ensured anonymity, confidentiality, and data protection. The study received ethical approval from an institutional ethics committee. With participants’ consent, all interviews were audio-recorded and subsequently transcribed verbatim. Field notes were produced after each interview to document contextual aspects, reflexive observations, and elements that could support the interpretation of participants’ narratives.
Data analysis followed the principles of Reflexive Thematic Analysis (Braun & Clarke, 2019), an approach that recognizes meanings in participants’ narratives as socially and contextually situated constructions shaped by power relations. The analytical process followed the six phases proposed by Braun and Clarke (2019): familiarization with the data, initial coding, theme generation and review, defining and naming themes, and reporting. MAXQDA (version 24) was used to organize and code the dataset.
Initial coding was conducted by the first author, and emerging themes were iteratively discussed with the co-authors throughout the analytic process, allowing for reflexive dialogue and refinement of interpretations grounded in the data. Throughout the analysis, a reflexive stance was maintained to ensure that themes emerged from participants’ narratives in dialogue with our theoretical framework, allowing for a critical and sensitive interpretation of their experiences.
Grounded in feminist and decolonial epistemologies, we engaged in ongoing reflexive practices, including memo writing and collaborative interpretation, to critically examine how our social locations influenced the research process. While shared language facilitated rapport, we remained attentive to power asymmetries. Rather than attempting to eliminate subjectivity, our reflexive stance aimed to make the conditions of knowledge production visible, thereby enhancing methodological rigor and ethical responsibility.
Results
From an intersectional, decolonial feminist, and social constructionist perspective (Collins & Bilge, 2021; Vergès, 2020), our analysis of participants' narratives revealed interconnected dimensions spanning their understandings of mental health, the difficulties faced, and the impact of migration. These data illustrate the complexity of Brazilian migrant women's experiences, shaped by interwoven individual, sociocultural, and institutional factors.
The analysis evidenced how accent, nationality, gender, and class operate alongside skin color in shaping the experiences participants brought to the interviews, producing distinct configurations of vulnerability and recognition across the sample. Through reflexive thematic analysis, these patterned meanings were organized into the themes and subthemes presented in Table 2.
Table 2.
Themes and subthemes
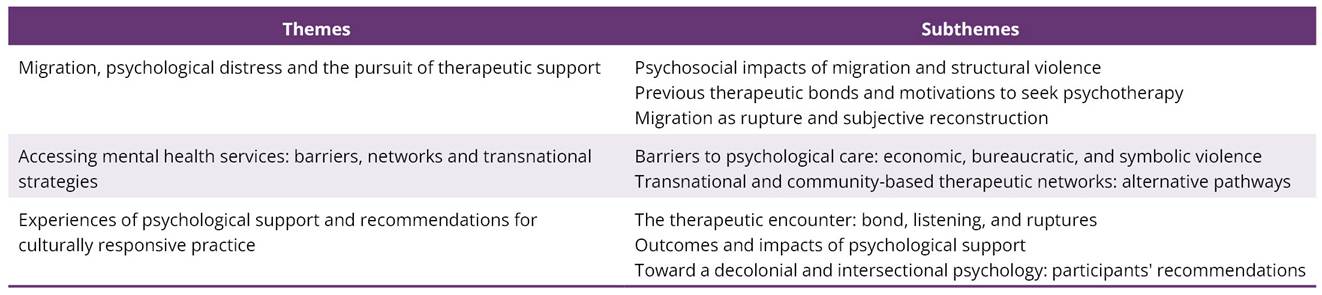
Note. Subthemes summarize recurrent patterns identified through reflexive thematic analysis (Braun & Clarke, 2019).
Migration, psychological distress and the pursuit of therapeutic support
Participants described the migratory experience as a transformative and ambivalent event, where gender, race, and migratory status emerge as inseparable dimensions that shape psychological distress and influence how psychological care is accessed or reconstructed.
Psychosocial impacts of migration and structural violence
Arriving in Portugal triggered new forms of suffering, marked by feelings of exclusion, loneliness, and difficulties adapting. Participants described challenges in forming social bonds and maintaining their identities:
"I became depressed because I didn't like the city, because I couldn't build relationships with people, people had no relationship with me" (IMG01).
"It is quite violent to have to stop being yourself in several situations, to hide or mask traits of your culture, your appearance, in order to adapt" (IMG06).
These strategies of identity silencing, often a response to racism and xenophobia, directly impact mental health. This connection between psychological distress and physical manifestations was evident in many narratives:
"I had a stress crisis, my eyelashes fell out, my eyebrows fell out… I stopped wearing makeup for almost a year" (IMG05).
"I had to stop the car and breathe, like: 'my God, I just need to breathe, it's really bad'" (IMG14).
Previous therapeutic bonds and motivations to seek psychotherapy
Among those who had already begun therapy before migrating, psychological support was perceived as crucial for facing the migratory process. A pre-existing therapeutic bond enabled them to anticipate and work through some of the most difficult aspects of migration:
"I already knew I would need therapy; I knew migration would not be easy (…) it was already in my mind: okay, I cannot drop therapy" (IMG06).
"Therapy helped me make the decision to leave my comfort zone and find the courage to migrate, because it was something I had always wanted to do but had never had the courage for" (IMG07).
Conversely, women who experienced frustrating encounters with therapists highlighted the discontinuity or inadequacy of the care they received:
"My first psychologist here was okay, but she was not aligned with what I needed; the second was incredible, she made a huge difference" (IMG11).
The primary motivation for seeking psychological support was most often linked to experiences of intense emotional distress, associated with professional devaluation, loss of social ties, institutional racism, and exhaustion:
I fell into a deep depression. I even thought it might be easier to disappear - that all of this would end if I were no longer here. But I felt I had to save myself. That's what made me seek psychological help. (IMG01)
"It was either go to therapy or smash a pile of plates and get fired" (IMG05).
The COVID-19 pandemic further intensified feelings of isolation and deepened psychological unease:
"It was a painful process for me, with the pandemic and everyone locked up at home, a chaotic environment. I had to look for a psychologist because I wasn't well" (IMG10).
In these contexts, therapy emerged as a way of preserving personal integrity amid great instability.
Migration as rupture and subjective reconstruction
Despite intense suffering, many participants reframed the migratory experience as an opportunity for subjective reconstruction and personal strengthening. For some, migration represented a chance to break with previous oppressive contexts and affirm new ways of existing. The rupture with familiar environments enabled processes of self-discovery and identity transformation:
"I'm no longer the same person. Migration is more of an intimate transformation. I looked inside myself for the first time" (IMG03).
I feel that here I grew much more. I needed to leave my context in São Paulo, even the church, to which I was very attached. This rupture brought me a perception that life is much more complex, with many experiences. It made me understand that my life is not limited to the city of São Paulo, the people there, or a church. That was important. (IMG09)
Migration also facilitated the construction of autonomy and personal agency, particularly in relation to family dynamics and social expectations:
"Now no one will shout at me, now no one will humiliate me" (IMG04).
It was a turning point in my life, this immigration. I finally managed to assert myself before my family. I am feeling stronger, firmer. I am a thirty-seven-year-old woman, I take the reins of my life, no one will tell me what to do. (IMG12)
The migratory process, while marked by adversity, also mobilized the development of resilience and emotional courage:
I feel that I am more resilient, that I have learned a lot about how to deal with people, with institutions. In terms of interculturality, I also learned a lot. This made me a more open person to the world, more fearless. I feel that today I throw myself more into things. (IMG06)
"Migration forced me to develop a strong capacity for agency; I am my greatest ally" (IMG08).
These narratives portray migration as an ambivalent phenomenon, simultaneously a source of stress and an opportunity for identity reconstruction. In navigating contexts of oppression, women mobilize resources of resistance, rebuilding ways of being and caring for themselves. The migratory experience thus emerges not as a linear trajectory, but as a complex process where suffering and empowerment coexist, challenging victimizing interpretations and affirming the political and subjective agency of migrant women.
Accessing mental health services: barriers, networks and transnational strategies
The pursuit of psychological support was shaped by multiple layers of suffering and the mobilization of diverse strategies to access care. Participants' narratives revealed a complex interplay between psychological distress, structural barriers, and support networks, which acted as mechanisms of resistance.
Barriers to psychological care: economic, bureaucratic, and symbolic violence
Participants described numerous obstacles in accessing psychological support, shaped by intersecting economic, bureaucratic, and symbolic dimensions. Some faced difficulties linked to documentation irregularities and a broader sense of institutional exclusion:
"I've always avoided anything public here, these are places where you get mistreated" (IMG09).
"I didn't have any documents, and even in terms of healthcare, it was complicated" (IMG12).
The cost of private therapy and finding professionals attuned to their experiences were also significant barriers. Many women reported interruptions in care due to being unable to afford it:
After a few sessions, I couldn't pay anymore (…) And another thing, I would bring up issues of sexism, racism, how important activism was in my life, how I needed to feel validated in certain matters, and I felt so undervalued. One time, the therapist even said something like: 'Well, not everything is sexism.' (IMG14)
The absence of culturally attuned listening and the dismissal of intersectional experiences compromised the continuity of care:
"The cultural, intersectional issue of being a woman, a migrant, racialized, it just wasn't a topic. And even if you raised it, they didn't know how to deal with it" (IMG02).
"She questioned my identity. I spoke about being a Black woman in Portugal and about situations of racism, and she downplayed it, that classic line: 'Oh, but you're not even that Black'" (IMG06).
These accounts highlight a widespread lack of preparedness among professionals in dealing with the psychological suffering of migrant women, whose experiences are frequently delegitimized. The scarcity of culturally competent professionals and inclusive therapeutic spaces perpetuate both suffering and inequalities in mental healthcare.
Transnational and community-based therapeutic networks: alternative pathways
Access to psychological support occurred through formal and informal contexts, including public services, private therapy, online groups, and grassroots collectives. Several participants reported mixed experiences with the National Health Service (SNS) and university settings, pointing to precarious conditions and difficulties in establishing a therapeutic bond:
I felt like I couldn't form a connection (...) there was so much demand, you know? So again, it was a question of precariousness, she couldn't attend to all the students who needed therapy, so appointments were really spaced out. I think that made it even harder to build that bond. (IMG10)
"I went to the public health service once and it didn't go very well. Even though my paperwork was fine, it's not a space I feel safe in" (IMG07).
Due to dissatisfaction with public services, many women sought alternatives in private or self-managed contexts. Group therapy and peer collectives were particularly valued for offering a sense of belonging and emotional containment:
"I've done group therapy before. And I really like it. It makes me feel great" (IMG03).
"I saw an ad on Facebook and sent a message and it worked out really well" (IMG09).
The identification with therapists who shared aspects of their identity (gender, race, nationality) was central to their choice. Black Brazilian women therapists, in particular, were seen as enabling more empathetic and non-hierarchical listening:
"I deliberately looked for a Black woman. Making that choice was important for me" (IMG06).
"My therapist is Brazilian and currently lives in England" (IMG08).
Even when supported by professionals who did not share their identities, some participants noted the value of being received without judgment:
"Even though she's Portuguese, a white woman, she is very welcoming... she doesn't invalidate what I bring" (IMG14).
These experiences demonstrate how a combination of informal networks, public and private services, and grassroots collectives constitute the repertoire of strategies migrant women use to access psychological support. The process was often difficult, particularly within the public healthcare system. Nonetheless, enablers like financial and emotional family support stood out:
"Always my family. So, having them to count on, receiving a monthly allowance for food, rent, and therapy, that was essential" (IMG09).
Moreover, community-based referrals were key resources for finding therapists with sensitive listening skills:
"It was a recommendation (…) I was in a really bad place, I needed help" (IMG08).
These narratives show that, despite institutional barriers, the mobilization of personal and collective networks plays a crucial role in securing care, becoming a form of collective resistance.
Experiences of psychological support and recommendations for culturally responsive practice
Participants' experiences with psychological support reveal a heterogeneous landscape, marked by stark contrasts between feelings of welcome and experiences of incomprehension. The quality of the therapeutic bond and cultural sensitivity were decisive in shaping the impact of the psychotherapeutic process.
Beyond describing their experiences, participants also articulated recommendations that express a desire for improvements in therapeutic practice and a collective critique of traditional psychology's limitations. They call for a culturally responsive psychological practice that is ethically and politically engaged.
The therapeutic encounter: bond, listening, and ruptures
The establishment of a therapeutic relationship was a central element in participants’ narratives, closely tied to empathic listening and the therapist's ability to understand the realities of migration. For some, the lack of cultural sensitivity and failure to recognize the specificities of life as racialized migrant women made it difficult to open up:
"I tried, but I couldn't open up. She's not going to understand my situation" (IMG04).
I remember the effort I made, and I don't think he really understood in the end (...) When I spoke about the migratory context, about being a woman here, Brazilian, not white, not with straight hair, when I brought all of that, I realized he didn't understand the weight it carried. (IMG07)
"I don't think I was able to build a bond. She was Portuguese too, right? Very different style from my first experience, and I ended up quitting therapy" (IMG15).
Conversely, where there were empathic listening and an effort to understand, even across identity differences, participants described powerful therapeutic connections:
"She understood everything I brought, or at least tried to understand, even though it was all far from her own reality" (IMG10).
"I still go to the same therapist today... she knows me well by now" (IMG13).
Aspects that facilitated positive experiences included continuity of care, professional empathy, a shared language, and therapeutic tools that supported emotional regulation:
"She was a very pleasant, kind, gentle person... so I was expecting her to be rude, but she wasn't" (IMG07).
"Now I have more tools... my therapy experiences have given me strategies to self-regulate" (IMG15).
However, many participants faced significant challenges, particularly when they felt their experiences were minimized or interpreted through a universalizing lens:
"There were a few situations where I felt bad... she minimized things... like, how could you have experienced racism if you're not even Black?'" (IMG07).
"It's really hard to walk in someone else's shoes when you haven't lived their reality" (IMG14).
Even where a positive bond was established, gaps in understanding the migratory experience persisted, exposing structural limitations of conventional psychological approaches:
"She doesn't really understand what it means to be a Latin American immigrant here in Portugal" (IMG09).
These perceptions underscore that, beyond empathy alone, multicultural competencies are essential for a truly transformative listening practice.
Outcomes and impacts of psychological support
The outcomes of psychological care varied considerably. In contexts marked by a lack of understanding, participants reported frustration, withdrawal, and a deepening sense of isolation:
"So, am I the one who's wrong then? It's not going to work out. I appreciate it, but no, it's not for me" (IMG04).
"It was terrible for me... I just started to give up on everything" (IMG07).
On the other hand, where an empathic bond was formed and the complexity of the migratory experience was acknowledged, the effects were overwhelmingly positive, promoting self-esteem, autonomy, and emotional maturity:
"It saved my life. I was able to realize my potential and embrace my complexity" (IMG09).
"Seeing how far we've come over time is really rewarding" (IMG13).
"Today, I'm a more emotionally regulated person" (IMG15).
These accounts highlight that the quality of the therapeutic bond and the practitioner’s intersectional sensitivity are crucial determinants of the impact that psychological care has in the lives of migrant women.
Toward a decolonial and intersectional psychology: participants’ recommendations
Participants stressed the need for professional training that recognizes the historical, social, and emotional dimensions of migration, moving away from decontextualized clinical models. They emphasized that psychological suffering cannot be understood in isolation from the structural violence embedded in their life trajectories:
"The social has to come into the clinic. Psychologists are too generalist (...) the impact of migration, of the social, and no one stops to think about that" (IMG01).
Women already come so battered... it's not just about where she's from, her nationality, her race, but about dealing with what she feels, seeing what's going on inside her (...) Knowing how to listen is one of the greatest professions in the world. (IMG02)
Their appeal is for a listening practice that is politically situated, critical, and intersectional, one that recognizes the colonial marks etched into the lives and bodies of migrant women. The decolonization of clinical practice was framed as an ethical imperative. Participants called on professionals to recognize their own positionalities and actively work to avoid reproducing racialized stereotypes:
"They need to decolonize psychological practice. Try to step out of your bubble" (IMG06).
"It's really important to pay attention and get past the stereotypes" (IMG09).
Decolonizing psychological care does not simply involve adding new content to curricula but adopting a clinical posture that legitimizes the knowledge of marginalized subjects and upholds practices that neither invisible nor pathologize their experiences. It is, above all, about transforming attitudes. Participants spoke of a cumulative build-up of exclusions and violence throughout their migratory journeys, which directly affects their mental health. They stressed that psychological care must acknowledge and address these multiple layers of suffering:
"Most of the situations women go through are cumulative (...) sometimes it builds up so much that we just break down" (IMG11).
According to them, clinical neutrality must be replaced by an ethical, empathic, and politically conscious mode of listening:
"Humanity, putting yourself in the other person's shoes... even just a little" (IMG04).
"Empathy should be basic, especially if someone works in mental health" (IMG13).
Shifting the clinical gaze towards a more critical mode of listening is essential for building therapeutic relationships that honor, rather than silence, their histories. Participants also drew attention to the emotional toll of navigating Portugal’s bureaucratic migration system. The erasure of the everyday struggles involved in legal processes was cited as a key factor that exacerbates psychological suffering:
"People have no idea what it's like, bureaucratically, to be a migrant... knowing that would make a difference" (IMG15).
Recognizing this as part of clinical listening is essential to avoid reducing suffering to individual pathology. Bureaucratic violence also produces harm:
Be empathetic, study, seek out different experiences, don't limit yourselves to what you already know. The more you expand, the more effective you'll be in working with diverse social realities. Validate what we bring, because we feel it. (IMG14)
Overall, the recommendations converge in advocating for a more critical and socially committed psychological practice that recognizes power asymmetries and the material conditions shaping the lives of migrant women. Their voices offer epistemological and ethical contributions that challenge clinical neutrality and advocate for a more situated and socially accountable approach. Developing multicultural and intersectional competencies is seen as key to creating therapeutic spaces that are genuinely welcoming and transformative.
Discussion
The pursuit of therapeutic support among racialized Brazilian immigrants in Portugal is a complex process shaped by structural and symbolic tension. Our findings demonstrate that difficulties in accessing psychological care and experiences of revictimisation in therapeutic settings are structurally produced through the intersections of gender, race, class, and nationality. Access to mental health services is permeated by intersectional inequalities that reproduce colonial hierarchies and structure the possibilities for listening, bonding and clinical validation (Collins & Bilge, 2021; Crenshaw, 2017; Kilomba, 2019; Rocha-Jiménez et al., 2025).
Participants' narratives revealed that the psychosocial impacts of migration are intrinsically tied to structural violence. The reported psychological distress, manifesting as anxiety, depression, and somatic symptoms, emerges from the precarity, bureaucratic barriers, and everyday violence faced in Portugal. This context is compounded by the rise of anti-migrant discourses and far-right parties, which intensify hostility faced by migrant populations (Stevens et al., 2024). These findings align with studies on the weight of post-migration conditions on migrants' mental health and demonstrate how intersecting social markers produce specific vulnerabilities (Collins & Bilge, 2021; Crenshaw, 2017).
For some participants, pre-existing therapeutic bonds from Brazil were crucial in navigating migration, enabling emotional stability, and developing coping strategies. This dimension of transnational therapeutic continuity represents an important contribution of this study, underscoring how migrants actively mobilize resources to sustain their well-being in contexts of structural adversity, a form of collective care and resilience in response to precarious labor conditions, discrimination, and institutional barriers (Teixeira et al., 2025; Azevedo et al., 2022). Seeking psychological support is a response to structural distress, often triggered by discrimination, precarious employment, and social vulnerabilities (Alarcão et al., 2024; Ryan et al., 2021; Teixeira et al., 2025), which were intensified by the COVID-19 pandemic.
However, the migratory experience is ambivalent. While migration to Portugal exposes women to new forms of structural violence, it also offers opportunities for emancipation and empowerment. This ambiguity (Azevedo et al., 2022) frames psychological distress as part of an identity-renegotiation process (Lantz et al., 2023). Despite intense suffering, many participants reframed migration as an opportunity for personal strengthening, challenging victimizing interpretations of their experiences.
Barriers to accessing mental health services reveal systematic exclusion, where financial, bureaucratic, symbolic, and cultural obstacles intersect (Inácio et al., 2025; Tourinho et al., 2024; Rocha-Jiménez et al., 2025). Despite the discourse of universality, reality is marked by long waiting lists, lack of information, and absence of policies for migrant populations (Inácio et al., 2025; Lin, 2023). The scarcity of multicultural psychologists reinforces a cycle of vulnerability that marginalizes Brazilian immigrants, reproducing racial and class hierarchies (Pussetti et al., 2009). These barriers are even more severe for migrants with irregular status (Stevens et al., 2024). Paradoxically, a shared language can reinforce subtle racism disguised as familiarity (França & Oliveira, 2021).
Among those who accessed care, experiences revealed deep gaps in cultural and structural competence. Difficulties in establishing therapeutic bonds often stem from clinicians' inability to recognize the weight of exclusion, racialization, and gender dynamics. Minimizing racism, individualizing social suffering, and reproducing stereotypes generate a dual process of silencing and revictimization (Inácio et al., 2025; Pussetti et al., 2009). The therapeutic setting can thus become a site of symbolic exclusion, echoing colonial practices (Kilomba, 2019; Vergès, 2020) and reproducing racial and power inequality (Barata, 2022; Pussetti et al., 2009; Radl-Karimi et al., 2022). The quality of the therapeutic encounter determines its outcome; where empathic bonds were formed, the effects were positive, promoting autonomy and emotional maturity. These accounts confirm that clinical competence cannot be dissociated from cultural and political awareness (Radl-Karimi et al., 2022).
In response, the participants developed creative transnational strategies. Seeking Brazilian psychologists online is a form of resistance that shifts the territorial logic of health systems, affirming their right to care and legitimizing their experiences. Shared language and cultural references facilitate a more immediate therapeutic connection. Family support was crucial in enabling access to private services. Recent studies indicate that technology-based interventions are associated with reductions in depressive and anxious symptoms among immigrants and refugees (Hynie et al., 2023). The importance of cultural and linguistic proximity in therapeutic relationships has been well documented, with research showing that culturally responsive care reduces unmet needs and improves service utilization (Lin, 2023). For Brazilian migrant women in Portugal, online therapy in Portuguese with therapists from Brazil constitutes not only a practical solution to institutional barriers but also a form of emotional validation and support amid linguistic, cultural, and institutional challenges.
These practices constitute distinctive epistemologies of care that challenge dominant Eurocentric models by creating transnational and community-based networks grounded in mutual validation (Pereira, 2022). Beyond individual psychotherapy, many turned to collectives and support groups, forming networks of communal care (Teixeira et al., 2025). By generating spaces of resistance outside institutions, these women challenge the power structures that perpetuate exclusion (Vergès, 2020), expand their care repertoires, and contest the monopoly of Western clinical psychology.
Our findings show that racialization in clinical encounters operates with differentiated intensities depending on the intersection of skin color with accent, nationality, gender, and class (Rocha-Jiménez et al., 2025; Teixeira et al., 2025). For Brazilian immigrants in Portugal, hypersexualized stereotypes circulate in therapeutic relationships, affecting bonding and treatment adherence (Barata, 2022; França & Oliveira, 2021), while the absence of culturally responsive mental health policies (Tourinho et al., 2024) leaves these dynamics institutionally unaddressed. Participants' recommendations converge in articulating a horizon of practice that displaces clinical neutrality and centers situated listening attuned to the material conditions shaping their lives. Their proposals do not call for technical refinement alone but for a reorganization of clinical attitudes capable of legitimizing the knowledge produced from positions historically marginalized within psychological discourse.
Final considerations
This study shows that racialized Brazilian immigrant women's experiences with psychological support in Portugal are shaped by intersecting structural inequalities rooted in gender, race, class, and nationality. Psychological distress emerges from material conditions of exclusion and precariousness, while migration operates as an ambivalent process, exposing women to new forms of structural violence while also enabling agency, identity reconstruction, and emotional recovery. Importantly, the pre-existing therapeutic bonds established in Brazil provided continuity of care for some participants, a dimension rarely addressed in research on migrant mental health.
By centering the voices of a population largely absent from Portuguese and international scholarship, this study advances an intersectional and decolonial understanding of migrant women's mental health. By focusing on the quality of the therapeutic encounter rather than solely on access or prevalence (Inácio et al., 2025; Tourinho et al., 2024), the analysis highlights creative resistance strategies, such as transnational therapy with Brazilian psychologists and community-based support networks that function as alternative epistemologies of care. These practices challenge Eurocentric assumptions about psychological support and contest the territorial and institutional boundaries of the national health systems. They are not merely compensatory responses to inadequate services; they constitute political acts that validate the experiences of migrant women and expand their care repertoires.
These findings further underscore that mental health is shaped by political and institutional conditions. Recognizing racialized migrant women's distress requires acknowledging the enduring effects of colonialism on clinical encounters, access to services, and therapeutic relationships (Kilomba, 2019; Vergès, 2020). When clinicians lack cultural and structural competence, individualize structural suffering, minimize racism, or reproduce stereotypes, the therapeutic setting becomes a site of symbolic exclusion. Conversely, when practitioners acknowledge migration as a complex and racialized process, psychotherapy fosters autonomy, self-esteem, and emotional stability among migrants. Clinical competence cannot be dissociated from cultural and political awareness; intersectional sensitivity is a crucial determinant of therapeutic efficacy.
The implications for practice and policy are significant. Participants' recommendations call for an urgent shift toward antiracist and decolonial clinical approaches capable of addressing distress in its structural dimension. This transformation requires more than adding multicultural content to curricula; it demands the reorientation of clinical attitudes, the development of critical reflexivity, and the legitimization of the knowledge of marginalized communities. Culturally responsive mental health policies must address the specific vulnerabilities of migrant populations, especially those with irregular status who face compounded bureaucratic and institutional violence. Recognizing these structural determinants is essential for building equitable and inclusive mental health systems.
Ultimately, this study demonstrates that migrant women are not passive recipients of care but active agents who challenge exclusionary systems and create alternative pathways to well-being. Their experiences offer ethical and epistemological contributions to the broader project of decolonizing mental health care. In an era marked by the rise of anti-immigrant rhetoric and the expansion of far-right movements across Europe (Stevens et al., 2024), acknowledging and supporting these forms of agency is timely and necessary for advancing justice in mental health care.
Limitations and directions for future research
This study has some limitations that suggest important directions for future research. The sample consisted of urban Brazilian women with stable digital access, which limits the transferability of the findings to migrants in rural areas or with fewer resources. Moreover, all participants were women who accessed some form of psychological support. Several were unable to enter the public mental health system and therefore paid for private therapy, underscoring how class-based barriers shape who can obtain care. Women who lacked both public access and financial means, arguably those facing the most severe structural exclusion, were not represented in this study.
Future research should include mental health professionals to identify gaps in multicultural and structural competence and further examine how class, race, and migration interact in clinical settings. Studies of transnational therapy networks and longitudinal and comparative research with other migrant groups would deepen our understanding of how racialization and colonial legacies shape access to psychological care. Such work is essential for advancing more inclusive and socially just mental health practices.
Acknowledgement
We are grateful to all the women who shared their stories.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government bodies, companies, private foundations, etc.) were declared for any aspect of the submitted work, including but not limited to grants and funding, advisory-board participation, study design, manuscript preparation, or statistical analysis.
Indexers
The Revista Psicologia, Diversidade e Saúde is indexed by DOAJ, EBSCO, Latindex – Catálogo 2.0 and LILACS.
Referencias
Alarcão, V., Candeias, P., Stefanovska Petkovska, M., Neves, J., Pintassilgo, S., Machado, F. L., Santos, O., Virgolino, A., Santos, R. R., Heitor, M. J., & Costa, A. (2024). Insights from the EQUALS4COVID19 study on migrant mental health in Portugal: A cross sectional mixed methods approach. BMC Public Health, 24, 2023. https://doi.org/10.1186/s12889-024-19563-x
Azevedo, L. F. D., França, T., & Cairns, D. (2022). Es mejor ser pobre aquí: Procesos de toma de decisiones sobre migración y consideraciones políticas y de estilo de vida entre brasileños calificados en Portugal [It is better to be poor here: Migration decision-making processes and political and lifestyle considerations among highly skilled Brazilians in Portugal]. Migraciones, 56, 1–16. https://doi.org/10.14422/mig.2022.020
Barata, C. (2022). “Mix of races, bad uterus”: Obstetric violence in the experiences of Afro Brazilian migrants in Portugal . Societies, 12(3), 78. https://doi.org/10.3390/soc12030078
Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health, 11(4), 589–597. https://doi.org/10.1080/2159676X.2019.1628806
Braun, V., & Clarke, V. (2021). Thematic analysis: A practical guide. SAGE Publications.
Collins, P. H., & Bilge, S. (2021). Interseccionalidade [Intersectionality]. Boitempo.
Crenshaw, K. W. (2017). On intersectionality: Essential writings. The New Press.
França, T., & Oliveira, S. P. (2021). Mulheres migrantes brasileiras como killjoys: Divulgando o racismo em Portugal “amigável” [Brazilian migrant women as killjoys: Exposing “friendly” racism in Portugal]. Revista Estudos Feministas, 29(1), e63001. https://doi.org/10.1590/18094449202100630001
Hynie, M., Oda, A., Calaresu, M., Kuo, B. C. H., Ives, N., Jaimes, A., Bokore, N., Beukeboom, C., Ahmad, F., Arya, N., Samuel, R., Farooqui, S., Palmer Dyer, J. L., & McKenzie, K. (2023). Access to virtual mental healthcare and support for refugee and immigrant groups: A scoping review. Journal of Immigrant and Minority Health, 25(5), 1171–1195. https://doi.org/10.1007/s10903-023-01521-1
Inácio, R., Gonçalves, R., Pires, J., Marques, M. J., & Dias, S. (2025). Access and utilisation of Portuguese mental healthcare services by migrant children and adolescents: Perceptions and experiences of families. Children and Youth Services Review, 178, 108535. https://doi.org/10.1016/j.childyouth.2025.108535
Kilomba, G. (2019). Memórias da plantação: Episódios de racismo cotidiano [Plantation memories: Episodes of everyday racism]. Cobogó.
Lantz, P. M., Goldberg, D. S., & Gollust, S. E. (2023). The perils of medicalization for population health and health equity. The Milbank Quarterly, 101(1), 61–82. https://doi.org/10.1111/1468-0009.12619
Lin, S. L. (2023). Inequities in mental health care facing racialized immigrant older adults with mental disorders despite universal coverage: A population based study in Canada. The Journals of Gerontology: Series B, 78(9), 1555–1571. https://doi.org/10.1093/geronb/gbad036
Pereira, D. F. (2022). Decolonialidade e avaliação psicológica [Decoloniality and psychological assessment]. Vozes.
Pussetti, C. (Coord.), Ferreira, J. F., Lechner, E., & Santinho, C. (2009). Migrantes e saúde mental: A construção da competência cultural [Migrants and mental health: The construction of cultural competence]. Alto Comissariado para a Imigração e Diálogo Intercultural.
Radl-Karimi, C., Nielsen, D. S., Sodemann, M., Batalden, P., & von Plessen, C. (2022). “When I feel safe, I dare to open up”: Immigrant and refugee patients’ experiences with coproducing healthcare. Patient Education and Counseling, 105, 2338–2345. https://doi.org/10.1016/j.pec.2021.11.009
Rocha-Jiménez, T., Torres, I., Cabieses, B., López Cevallos, D. F., & Mercado Órdenes, M. (2025). Intersectionality, racism, and mental health of migrants arriving at borders in Latin America: A qualitative study based on in depth interviews with key informants of the cases of Ecuador and Chile. The Lancet Regional Health – Americas, 44, 101040. https://doi.org/10.1016/j.lana.2025.101040
Rogers, W. S., & Willig, C. (Eds.). (2017). The SAGE handbook of qualitative research in psychology (2nd ed.). SAGE Publications.
Ryan, D., Tornberg Belanger, S. N., Perez, G., Maurer, S., Price, C., Rao, D., Chan, K. C. G., & Ornelas, I. J. (2021). Stress, social support and their relationship to depression and anxiety among Latina immigrant women. Journal of Psychosomatic Research, 149, 110588. https://doi.org/10.1016/j.jpsychores.2021.110588
Stevens, A. J., Boukari, Y., English, S., Kadir, A., Kumar, B. N., & Devakumar, D. (2024). Discriminatory, racist and xenophobic policies and practices against child refugees, asylum seekers, and undocumented migrants in European health systems. The Lancet Regional Health – Europe, 41, 100834. https://doi.org/10.1016/j.lanepe.2023.100834
Teixeira, I. N., Silva, P., Alckmin Carvalho, F., & Padilla, B. (2025). “We help each other through it”: Community support and labor experiences among Brazilian immigrants in Portugal. Behavioral Sciences, 15(9), 1283. https://doi.org/10.3390/bs15091283
Tong, A., Sainsbury, P., & Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): A 32 item checklist for interviews and focus groups. International Journal for Quality in Health Care, 19(6), 349–357. https://doi.org/10.1093/intqhc/mzm042
Torlig, E. G. S., Resende Junior, P. C., Fujihara, R. K., Montezano, L., & Demo, G. (2022). Proposta de validação para instrumentos de pesquisa qualitativa (Vali Quali) [Proposal for validation of qualitative research instruments (Vali Quali)]. Administração Ensino e Pesquisa, 23(1), 5–31. https://doi.org/10.13058/raep.2022.v23n1.2022
Tourinho, L. O. S., Sotero, A. P. S., & Rodríguez, P. G. (2024). Migrações forçadas de mulheres e meninas e o direito à saúde: Uma análise comparada das experiências do Brasil, Espanha e Portugal [Forced migrations of women and girls and the right to health: A comparative analysis of experiences in Brazil, Spain, and Portugal]. Cuadernos de Educación y Desarrollo, 16(16), Artículo e162024104. https://doi.org/10.61541/hhesqd76
Vergès, F. (2020). Um feminismo decolonial [A decolonial feminism]. Ubu.
World Health Organization. (2025, September). Refugee and migrant mental health. https://www.who.int/news-room/fact-sheets/detail/refugee-and-migrant-mental-health
Appendix
Semistructured interview guide
Experiences of Immigrant and Racialized Women Regarding Psychological Support Received in Portugal
Welcome
Welcome the participant, explain the study’s purpose, and reinforce that participation is voluntary. Explain that the recording will only be used for transcription purposes. Data collected will be kept confidential, and no information that could identify the participant will be recorded. The results will be used solely for research purposes. Start recording and request oral consent.
1. SEMISTRUCTURED INTERVIEW
Psychological Health
How would you assess your current mental health?
Did you access any mental health services in Brazil? If yes, which ones and how was the experience (e.g., psychotherapy, psychiatric care)?
If you had support in Brazil, at the time, did you find it useful? How?
Has immigration to Portugal affected your mental health? If yes, in what ways?
Which aspects of the migration process do you consider to have most affected your psychological wellbeing (e.g., homesickness, cultural adaptation, financial difficulties)?
Have you experienced any particularly difficult moments since your arrival? How did you cope with them?
Have you faced any discrimination in Portugal for being a woman, immigrant, and/or racialized (e.g., racism, xenophobia, prejudice)? Could you describe some situations?
How did these situations make you feel? Did you seek help or support afterward? If yes, from whom and how was the support received?
How do you think these experiences may have affected your psychological wellbeing and integration process?
Do you know other immigrant and racialized women who have had similar experiences?
Are there any support networks or groups you attend or would recommend to others in similar situations?
Psychological Support
What motivated you to seek psychological support here in Portugal?
How was the process of finding and accessing these services? Where did you receive care and how was your experience (e.g., public service, private practice, institutions)?
What were your main complaints or demands?
Do you think the psychologist was prepared to address your needs?
Do you think the psychologist was personally prepared to work with racialized immigrant populations?
What are your thoughts on the influence of psychologists’ personal beliefs and values on interventions with immigrant and racialized people?
During psychological support, did you experience any moments you consider:
◦Challenging? If yes, can you describe them?
◦Rewarding? If yes, can you describe them?
Did the psychological support have significant impacts on your life? If yes, what were the effects?
Multicultural Competencies and Recommendations
As an immigrant and racialized woman, what recommendations would you give to psychologists working with this population?
Is there any other point you would like to include? Any aspect of your experience you wish to share?
Is there any topic we haven’t addressed but that you consider important to mention?
Interview conducted on: __/____/____ Duration of interview: __________
SOCIODEMOGRAPHIC DATA
Age: ______
Education: __________________
Marital status: ____________________
Gender identity: ___________________
Sexual orientation: _________________
Ethnic-racial identity (e.g., White, Black, Yellow, Indigenous): ______________________
Place of birth: ___________________
Nationality: ________________________
Occupation/profession: ___________________
Currently working? __________
Length of residence in Portugal: _____
With this, the interview concludes. Thank you again for your participation, which is extremely valuable and will certainly enrich this study.
FIELD NOTES
During the interview, notes will be taken regarding objective elements (location and time of the interview) and subjective aspects that arise, such as non-verbal cues, emotional state, silences, possible discomfort, or difficulties discussing a topic, in order to contextualize the interview for later analysis.
