Original article
Correlation between biomechanical parameters, pelvic morphometry, and risk factors for urinary incontinence in older women: a dynamic magnetic resonance imaging study / Correlação entre parâmetros biomecânicos, morfometria pélvica e fatores de risco para incontinência urinária em idosas: um estudo por ressonância magnética dinâmica
Mariana Santos de Lucca1 (https://orcid.org/0009-0002-9697-9382)
Rubia Motta da Silva2 (https://orcid.org/0000-0001-5335-5671)
Maycon Sousa Pegorari3 (https://orcid.org/0000-0003-4015-9895)
Karla Helena Vilaça e Silva4 (https://orcid.org/0000-0002-4937-2396)
Eduardo Ferriolli5 (https://orcid.org/0000-0002-5028-2451)
Lislei Patrizzi6 (https://orcid.org/0000-0002-3729-7675)
1-3Universidade Federal do Triângulo Mineiro (Uberaba). Minas Gerais, Brazil.
4Universidade Católica de Brasília (Brasília). Distrito Federal, Brazil.
5Universidade de São Paulo (Ribeirão Preto). São Paulo, Brazil.
6Corresponding contact. Universidade Federal do Triângulo Mineiro (Uberaba). Minas Gerais, Brazil. [email protected]
ABSTRACT | INTRODUCTION: Urinary continence depends on the interaction between muscular, ligamentous, and biomechanical structures that support the bladder and urethra. Morphometric and postural parameters, such as lumbosacral and pelvic angles, pelvic floor-to-bladder distances, and anatomical diameters, help to understand this support, while outcomes like bladder displacement and pelvic floor muscle contractile response reflect its functionality. Failures in this interaction constitute predisposing factors for urinary incontinence (UI) in older women. OBJECTIVE: To analyze the correlation between pelvic and lumbosacral morphometric measures and predisposing factors for urinary incontinence in older women. METHODS: This cross-sectional observational study included 22 women over 60 years of age (mean 71.5 years). The participants were assessed using dynamic magnetic resonance imaging to measure pelvic and lumbosacral angles and distances, and by surface electromyography to evaluate the contractile response of the pelvic floor muscles. Associations were analyzed using Pearson’s and Spearman’s correlation coefficients, adopting a 5% significance level. RESULTS: Correlation analyses revealed a positive association between body mass index and pubococcygeal distance (r = 0.463). Conversely, negative correlations were observed between age and pelvic inclination angle (PIA) (r = -0.476), between PIA and UI (r = -0.448), between the anteroposterior diameter (APD) and the presence of UI (r = -0.543), between the lumbosacral angle (LSA) and PIA (r = -0.433), and between maximum non-sustained contraction (NSC) and the pelvic floor-to-bladder distance during straining (PFBD-S) (r = -0.485). CONCLUSION: In older women, morphometric measures of the pelvis and lumbosacral region show significant associations with predisposing factors for urinary incontinence. The interaction between structural support and pelvic floor muscle functionality appears to be a key determinant of urinary continence, highlighting the importance of comprehensive physiotherapeutic assessments that consider both morphometric parameters and contractile muscle response.
KEYWORDS: Urinary Incontinence. Pelvic Floor Disorders. Pelvis. Lumbosacral Region. Aged. Women. Magnetic Resonance Imaging.
RESUMO | INTRODUÇÃO: A continência urinária depende da interação entre estruturas musculares, ligamentares e biomecânicas que sustentam a bexiga e a uretra. Parâmetros morfométricos e posturais, como ângulos lombossacral e pélvico, distâncias do assoalho pélvico à bexiga e diâmetros anatômicos, ajudam a compreender esse suporte, enquanto desfechos como deslocamento vesical e resposta contrátil do assoalho pélvico refletem sua funcionalidade. Falhas nessa interação constituem fatores predisponentes para a incontinência urinária (IU) em mulheres idosas. OBJETIVOS: analisar a correlação entre medidas morfométricas da pelve e da região lombossacral, com fatores predisponentes para a incontinência urinária em mulheres idosas. MÉTODOS: Estudo observacional transversal realizado com 22 mulheres com idade superior a 60 anos (média de 71,5 anos). As participantes foram avaliadas por ressonância magnética dinâmica para mensuração dos ângulos e distâncias pélvicas e lombossacrais e por eletromiografia de superfície para avaliação da resposta contrátil dos músculos do assoalho pélvico. As associações foram analisadas por meio dos coeficientes de correlação de Pearson e Spearman, adotando-se nível de significância de 5%. RESULTADOS: As análises de correlação evidenciaram associação positiva entre o índice de massa corporal e a distância pubococcígea (r = 0,463). Em contrapartida, observaram-se correlações negativas entre a idade e o ângulo de inclinação pélvica (AIP) (r = -0,476), AIP e IU (r = -0,448) entre o diâmetro ântero-posterior (DAP) e a presença de IU (r = -0,543), entre o ângulo lombossacral (ALS) e o AIP (r = -0,433), e entre a contração máxima não sustentada (CM-NS) e a distância assoalho-bexiga em esforço (DAB-E) (r = -0,485). CONCLUSÃO: Em mulheres idosas, medidas morfométricas da pelve e da região lombossacral apresentam associações significativas com fatores predisponentes para a incontinência urinária. A interação entre suporte estrutural e funcionalidade do assoalho pélvico parece ser determinante para a continência urinária, reforçando a importância de avaliações fisioterapêuticas integradas que considerem tanto parâmetros morfométricos quanto a resposta contrátil muscular.
PALAVRAS-CHAVE: Incontinência Urinária. Distúrbios do Assoalho Pélvico. Pelve. Região Lombossacral. Idoso. Mulheres. Imageamento por Ressonância Magnética.
How to cite this article: Lucca MC, Silva RM, Pegorari MS, Silva KHV, Ferriolli E, Patrizzi L. Correlation between biomechanical parameters, pelvic morphometry, and risk factors for urinary incontinence in older women: a dynamic magnetic resonance imaging study. J Physiother Res. 2026;16:e6679. https://doi.org/10.17267/2238-2704rpf.2026.e6679
Submitted Dec. 23, 2025, Accepted Apr. 14, 2025, Published June 2, 2026
J. Physiother. Res., Salvador, 2026;16:e6679
https://doi.org/10.17267/2238-2704rpf.2026.e6679
ISSN: 2238-2704
Assigned editor: Juliana Goulardins
1. Introduction
The maintenance of urinary continence depends on an integrated system of musculoskeletal and support structures, functionally interdependent, as well as on biomechanical parameters that modulate the positioning and stability of the bladder and urethra1. Among these variables, the lumbosacral angle (LSA), pelvic inclination angle (PIA), pelvic floor–to–bladder distance at rest (PFBD-R) and during effort (PFBD-E), anteroposterior diameter (APD), pubococcygeal distance (PCD), and anovulvar distance (AVD) stand out, all of which are essential for understanding bladder support and pelvic floor function.
The LSA determines sacral inclination relative to the lumbar spine, influencing the force vector transmitted by intra-abdominal pressure. Changes in this orientation may alter load transmission to the pelvis, with potential repercussions on the pelvic floor during effort2. Studies on sacral inclination suggest that a more vertical sacrum may modify the vector of loads transmitted to the pelvis, potentially increasing demand on the pelvic floor during effort. Conversely, a more horizontal sacral orientation tends to favor more efficient force distribution, contributing to bladder and urethral support3,4.
The PIA reflects the global orientation of the pelvis, directly influencing bladder positioning and tension applied to perineal structures. Pelvic retroversion displaces the bladder inferiorly and increases urethral hypermobility, which is associated with a higher risk of stress urinary incontinence, whereas anteversion facilitates a more favorable angle for urethral closure and improves the stabilizing action of pelvic musculature1,4.
The PFBD-R and PFBD-E distances provide precise indicators of bladder support. PFBD-R reflects support at rest, whereas PFBD-E indicates bladder neck mobility in response to increased intra-abdominal pressure. A marked increase in PFBD-E is typical in women with stress urinary incontinence, as it reflects the inability of the pelvic floor to contract synchronously and stabilize the bladder during effort5.
APD, PCD, and AVD measurements complement the functional analysis by reflecting the volume, tone, and degree of separation between anatomical structures of the pelvic floor. The bony pelvis constitutes the structural framework within which the pelvic organs (bladder, urethra, vaginal canal, and rectum) are suspended and stabilized by a complex musculofascial system. The configuration of this bony structure influences how forces act on the pelvic floor during functional activities. A deeper bony pelvis, characterized by a greater APD between the sacral promontory and the superior margin of the pubic symphysis, may redistribute gravitational force vectors and the transmission of intra-abdominal pressures, reducing the concentration of loads on the urogenital hiatus and favoring their dissipation within the pelvic cavity. This structural arrangement may positively influence load distribution across the pelvic floor muscles and the mechanisms of urethral and bladder support, creating a biomechanical environment more favorable for the function of the support network described by the Hammock Hypothesis6-8.
Although the anteroposterior dimension of the pelvis does not act directly as a urinary continence mechanism, it conditions the biomechanical environment in which muscular, fascial, and ligamentous systems operate, potentially influencing, indirectly, urethral coaptation efficiency and pelvic health maintenance, especially when associated with factors such as aging, parity, and muscle function alterations6-8.
The PCD, which measures the distance between the pubis and coccyx, reflects the degree of stretching of deep musculature and supporting ligaments, and may increase in conditions of muscle weakness or chronic abdominal pressure9.
The AVD, corresponding to the distance between the anus and vulvar commissure, is an important marker of perineal integrity; reductions in this measure have been associated with increased mechanical demand on the sphincter and higher risk of dysfunctions, while higher values may reflect greater separation of urethral and bladder support structures10,11.
Although this approach is based on mechanisms involved in maintaining urinary continence, it is fundamental for understanding urinary incontinence as a clinical manifestation of failure in pelvic floor support and control systems. The literature predominantly describes these parameters in isolation, with emphasis on clinical or static assessments, and there is a lack of studies investigating, in an integrated and dynamic manner, the relation between lumbosacral and pelvic morphometric measures and urinary incontinence in this population.
In this context, dynamic magnetic resonance imaging may broaden this understanding by enabling simultaneous evaluation of relations between osteomuscular and visceral structures under functional conditions.
The integration of these parameters demonstrates that postural changes, insufficient anatomical support, and increased bladder mobility compose a biomechanical scenario conducive to the development of urinary incontinence. Thus, the assessment of LSA, PIA, PFBD-R, PFBD-E, APD, PCD, and AVD should be considered in pelvic physiotherapy clinical practice, as it allows targeted interventions aimed at pelvic realignment, improved muscle function, and optimization of bladder support.
The hypothesis was that pelvic and lumbosacral biomechanical parameters in older women favor urinary incontinence. It was assumed that lower bladder neck mobility during effort, reflected by lower PFBD-E values, as well as lower PCD and higher AVD, would be associated with greater integrity and better support of pelvic floor structures. It was also assumed that more appropriate LSA and PIA values would be associated with better distribution of intra-abdominal forces and more efficient bladder support. Finally, it was considered that a greater APD would be related to a more favorable biomechanical environment, contributing to the maintenance of urinary continence.
Therefore, the aim of this study was to analyze the correlation between pelvic and lumbosacral morphometric measures and predisposing factors for urinary incontinence in older women.
2. Materials and methods
This is an observational, cross-sectional study with an exploratory approach, approved by the Research Ethics Committee under protocol HCRP (opinions nº 15338/2005 and 1256/2006). The study included a convenience sample of older women randomly recruited from the Gynecology and Obstetrics Outpatient Clinic of the University Hospital of the Ribeirão Preto Medical School (Hospital Universitário da Faculdade de Medicina de Ribeirão Preto), University of São Paulo (Universidade de São Paulo), according to established eligibility criteria. Of 130 women approached, 60 agreed to participate and met inclusion criteria. However, 38 were excluded for not completing all assessments, resulting in a final sample of 22 women aged over 65 years (mean 71.5 years; range 65–84 years). All participants signed the informed consent form, and data collection began after ethics approval (July/2025 to September/2026).
2.1 Inclusion and exclusion criteria
Women aged 60 years or older were included in the study. Exclusion criteria comprised a history of neurological diseases, previous surgical interventions involving the genitourinary system within the last 10 years, presence of a pacemaker, cardiac valve, aneurysm, or angioplasty within the previous 3 months, use of prostheses or similar devices, self-reported claustrophobia, and contraindications to magnetic resonance imaging (MRI).
2.2 Procedures adopted for each stage of the protocol
Participants underwent a clinical and functional assessment consisting of three stages. In stage 1, height and weight were measured to calculate body mass index (BMI), and complaints of urinary incontinence were assessed. The presence of urinary incontinence was determined by self-report. Prior to data collection, participants received standardized information regarding the concept of urinary incontinence, adopting the definition of the International Continence Society (ICS), which defines it as any involuntary loss of urine. Following this explanation, participants were classified according to the presence or absence of urinary incontinence. In stage 2, surface electromyography (EMG) was performed using the Phenix USB2 device (CCE, UZ), with a reference self-adhesive electrode and an intracavitary (vaginal) electrode. Initially, all participants were instructed on how to correctly perform pelvic floor muscle contractions. Subsequently, the V03 R8 software recorded four non-sustained contractions (5-second intervals) and four sustained contractions lasting ten seconds (20-second intervals), totaling 120 seconds of recording for each participant. Additionally, a physical examination was conducted in this stage to determine the anovulvar distance (AVD). Finally, in stage 3, magnetic resonance imaging (MRI) was performed using a 1.5 Tesla Magnetom Vision scanner (Siemens, Erlangen, Germany) with a 6-channel phased-array pelvic coil. Static images were acquired in axial, coronal, and sagittal planes (T1- and T2-weighted), as well as dynamic sagittal images at rest and during effort (Valsalva maneuver and isometric contraction), T2-weighted. The following parameters were evaluated: lumbosacral angle (LSA), pelvic inclination angle (PIA), pelvic floor–to–bladder distance at rest (PFBD-R) and during effort (PFBD-E), as well as morphometric parameters including anteroposterior diameter (APD) and pubococcygeal distance (PCD), all of which are essential for understanding bladder support and pelvic floor function.
Figure 1. Lumbosacral angle (LSA)

Figure 2. Pelvic inclination angle (PIA)

Figure 3. Pelvic floor–to–bladder distance at rest (PFBD-R)
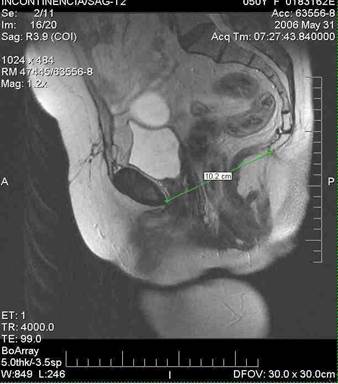
Figure 4. Pelvic floor–to–bladder distance during effort (PFBD-E)
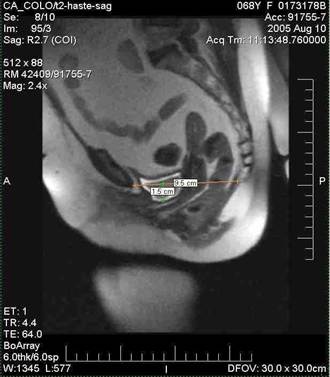
Figure 5. Anteroposterior diameter (APD)

Figure 6. Pubococcygeal distance (PCD)

The independent variables of the study included morphometric and postural measures of the pelvis and the lumbosacral region, such as LSA, PIA, PFBD-R and PFBD-E, APD, PCD and AVD, as well as anthropometric data, such as age and body mass index.
The dependent variables (outcomes) corresponded to pelvic floor functionality and urinary continence, assessed by bladder displacement during effort, measured by dynamic magnetic resonance imaging, and by the contractile response of the pelvic floor muscles, assessed by surface electromyography.
2.3 Statistical analysis
Quantitative numerical variables were described as mean and standard deviation. Correlations between quantitative variables with parametric distribution were evaluated using Pearson’s correlation coefficient, whereas for variables with non-parametric distribution, as well as for the correlation between quantitative variables and the presence of urinary incontinence, Spearman’s correlation coefficient was used, adopting a significance level of 5%. For interpretation of the magnitude of correlations, values between 0.70 and 1.00 were considered strong, between 0.40 and 0.60 moderate, and between 0.10 and 0.30 weak12. The data were processed and statistically analyzed using SPSS Statistics® software, version 22.
3. Results
Women aged between 60 and 84 years participated in the study, with a mean age of 71.59 (±6.45) years. BMI ranged from 20.39 to 37.97 kg/m², with a mean of 29.89 (±4.37) kg/m². Of the total of 22 women evaluated, 15 (68.2%) presented urinary incontinence. The measurements obtained in the sample are presented in table 1.
Table 1. Clinical, anthropometric, electromyographic, and morphometric characteristics of the participants (n = 22)
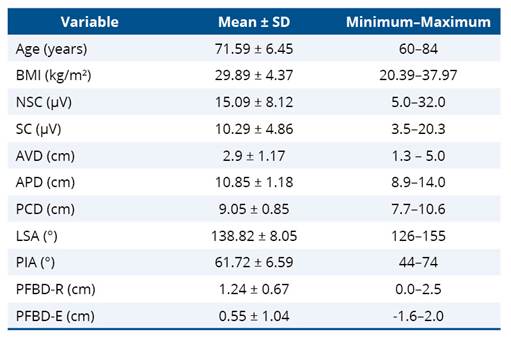
BMI - body mass index; NSC - non-sustained muscle contraction; SC - sustained muscle contraction; AVD - anovulvar distance; APD - anteroposterior diameter; PCD - pubococcygeal distance; LSA - lumbosacral angle; PIA - pelvic inclination angle; PFBD-R - pelvic floor–to–bladder distance at rest; PFBD-E - pelvic floor–to–bladder distance during effort; SD - standard deviation.
Correlation analyses showed a positive association between BMI and PCD, suggesting that higher body mass index values are associated with greater pubococcygeal distance. Age showed a negative correlation with PIA, indicating pelvic retroversion with advancing age, and PIA showed a negative correlation with UI, suggesting that lower values of the pelvic inclination angle were associated with the presence of urinary incontinence.
There was a negative correlation between LSA and PIA, suggesting that an increase in the lumbosacral angle was associated with a reduction in the pelvic inclination angle. NSC was negatively correlated with PFBD-E, indicating that greater non-sustained muscle contraction capacity was associated with lower bladder mobility during effort. In addition, a positive correlation was identified between SC and BMI, suggesting that higher body mass index values were associated with greater sustained muscle contraction values.
Muscle function measures showed a strong correlation between SC and NSC, suggesting functional integration between non-sustained and sustained pelvic floor contractions. A negative correlation was observed between APD and UI, indicating that lower values of the anteroposterior diameter of the pelvis were associated with the presence of urinary incontinence. Additionally, AVD and APD showed a positive correlation, suggesting that higher values of the anovulvar distance were related to greater anteroposterior pelvic dimensions.
Table 2. Correlations between clinical, electromyographic, biomechanical, and morphometric variables of the sample
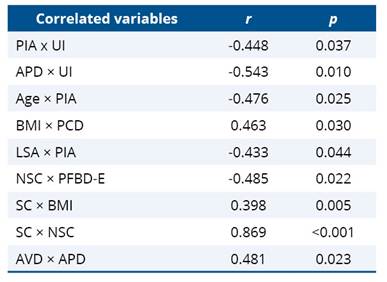
PIA - pelvic inclination angle (°); UI - urinary incontinence; APD - anteroposterior diameter (cm); BMI - body mass index (kg/m²); PCD - pubococcygeal distance (cm); LSA - lumbosacral angle (°); NSC - non-sustained muscle contraction (µV); PFBD-E - pelvic floor–to–bladder distance during effort (cm); SC - sustained muscle contraction (µV); AVD - anovulvar distance (cm).
Graphic 1. Correlations between pelvic and lumbosacral distance and angle measures, urinary incontinence, pelvic floor muscle contraction, BMI, and age
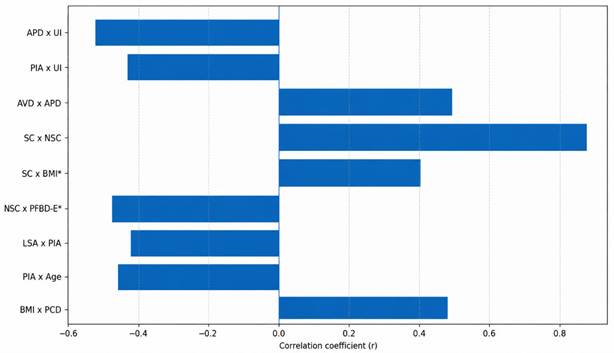
APD - anteroposterior diameter; UI - urinary incontinence; PIA - pelvic inclination angle; AVD - anovulvar distance; SC - sustained muscle contraction; NSC - non-sustained muscle contraction; BMI - body mass index (kg/m²); PFBD-E - pelvic floor–to–bladder distance during effort; LSA - lumbosacral angle; PCD - pubococcygeal distance.
*Spearman correlation.
4. Discussion
In the present study, older women were analyzed, considering anthropometric, morphometric, and postural parameters of the pelvis and the lumbosacral region. The independent variables included age, body mass index, and morphometric and postural measures of the pelvis and lumbosacral spine, while the dependent variables corresponded to urinary continence outcomes, such as bladder displacement during effort, contractile response of the pelvic floor muscles, and the clinical presence of urinary incontinence.
The associations are observational, without inference of causality, highlighting the need for caution when extrapolating the results to populations with characteristics different from those analyzed.
The findings of this study demonstrate that anthropometric, postural, and morphometric parameters of the pelvic floor are interrelated in a relevant manner for understanding bladder support and urinary continence. It was observed that an increase in pubococcygeal distance tends to occur in individuals with higher anthropometric indices13,14.
This association supports the understanding that increased intra-abdominal pressure, often present in individuals with higher body mass, may result in chronic stretching of the muscular and ligamentous components of the pelvic floor, promoting their separation and reducing the mechanical efficiency of urethral support. This mechanism has been previously described by Dietz, who highlights the impact of abdominal overload on pelvic morphology and the mobility of pelvic organs15.
The relation between age and the pelvic inclination angle reinforces the influence of aging on pelvic positioning. The literature shows that senescence is associated with musculoskeletal changes, including alterations in pelvic alignment and reduced lumbosacral stabilization capacity. Such changes may impact bladder positioning and the functioning of continence mechanisms, particularly due to increased urethral mobility and decreased reflex response of the deep musculature1,4,16.
Another relevant finding concerns the association between the lumbosacral angle and the pelvic inclination angle. The literature suggests that sacrolumbar alignment modulates the direction and magnitude of forces transmitted by intra-abdominal pressure3,4. Thus, changes in sacral positioning may modify the load vector applied to the bladder, influencing both support at rest and stability during effort. This biomechanical relation reinforces the importance of lumbopelvic interaction in maintaining continence, as discussed by authors who highlight the synergy between posture and pelvic floor function15.
The negative correlation identified between the PIA and LSA indicates that, in the analyzed sample, an increase in pelvic inclination in the sagittal plane occurred simultaneously with a reduction in sacral inclination relative to the lumbar spine.
Although these parameters are anatomically interrelated, their variation is not necessarily linear, especially in clinical situations in which sacroiliac joint mobility, lumbosacral stiffness, or compensatory postural patterns influence segmental behavior. Thus, even with the pelvis in anteversion—a condition in which greater sacral horizontalization would theoretically be expected—a tendency toward sacral verticalization was observed, resulting in a decrease in LSA1,3,4.
This phenomenon may reflect compensatory mechanisms aimed at maintaining trunk balance, notably through increased lumbar lordosis or limitation of sacral movement, factors that independently modulate the orientation of the pelvis and sacrum. This finding reinforces that adjustments between the pelvis and lumbar spine depend not only on global pelvic rotation but also on the interaction between paravertebral musculature, sacroiliac ligaments, and individual postural alignment characteristics, thus explaining the inverse relation observed between PIA and LSA17,18.
The observation of a negative correlation between PIA and symptoms of UI represents a distinctive and clinically relevant finding of this study. Considering that pelvic anteversion facilitates the pressure response of the pelvic floor, the identification of lower angles (greater anterior inclination) in patients with muscle distension (MD) and UI confirms the interdependence between muscular integrity and postural alignment. Such anterior displacement of the pelvis, associated with posterior trunk compensation, reflects a biomechanical strategy to optimize urethral closure in functionally compromised pelvic floors19,20. Subsequent studies, including dynamic imaging analyses and functional measurements, also suggest that changes in the pelvic sagittal plane influence the resting position of the bladder neck and the efficiency of the urethral closure mechanism, supporting the notion that moderate pelvic anteversion may be associated with reduced urethral displacement during effort7,21.
In contrast, a more posteriorly positioned pelvis or one with reduced inclination in the sagittal plane may decrease the effectiveness of the so-called urethral “support hammock”, predisposing to greater bladder neck mobility and reduced resistance to involuntary urinary flow, especially under conditions of increased intra-abdominal pressure, such as coughing or physical exercise6-10. These findings are consistent with sophisticated biomechanical models that consider sagittal pelvic geometry as a determinant of the relation between intra-abdominal forces and pelvic floor response22.
The relation between perineometric measures and bladder mobility during effort suggests that lower muscle contraction strength may be associated with greater displacement of the bladder neck. This finding is consistent with the model described by DeLancey, according to which urethral support depends on the integrity of the levator ani muscles and their ability to produce effective compression of the urethra during increases in intra-abdominal pressure6. Thus, impairments in muscle strength may facilitate urethral instability and contribute to symptoms of stress urinary incontinence.
When the anteroposterior diameter is considered from a bony structural perspective, defined as the distance between the sacral promontory and the superior margin of the pubic symphysis, its increase should not be interpreted as a direct risk factor for urinary incontinence. On the contrary, a greater anteroposterior depth of the pelvis may reflect a bony architecture more favorable for the redistribution of intra-abdominal pressures, reducing the concentration of loads on the urogenital hiatus and the distal continence mechanisms.
From a biomechanical perspective, this configuration may optimize the transmission of abdominal pressure to the proximal urethra, as described in the urethral support “hammock” model, in which continence depends on the efficient interaction between the urethra, supporting fasciae, and the pelvic floor. Thus, provided that muscular and fascial components are functionally preserved, a greater anteroposterior diameter of the bony pelvis may act as a potentially protective structural factor, contributing to the lower rates of urinary incontinence observed6,7,19.
The relation between the anteroposterior diameter, the anovulvar distance, and urinary incontinence can be understood as a structural–functional interaction between the bony framework, distal support, and the urethral support network. Urinary continence depends on the compression of the urethra against a network formed by the pelvic floor muscles, fasciae, and supporting ligaments. During increases in intra-abdominal pressure, the urethra is stabilized and compressed against this network, promoting efficient urethral closure. The integrity of this network is therefore essential for the maintenance of continence6.
The anovulvar distance, in turn, reflects the integrity of the perineal body, a central structure of distal pelvic floor support and an anchoring point for the muscles and fasciae involved in the formation of the urethral hammock. A functional anovulvar distance, generally within an intermediate range, favors tissue coaptation and adequate dissipation of intra-abdominal pressures, contributing to the stability of urethral support. In contrast, excessively increased anovulvar distances indicate distension or injury of the perineal body, compromising the efficiency of the support network and increasing the likelihood of urethral closure failure during effort8.
Thus, urinary incontinence emerges not from the isolated behavior of a single morphometric measure, but from the relation between the anteroposterior depth of the bony pelvis and the functional integrity of distal support, represented by the anovulvar distance. When these two dimensions are balanced and associated with functionally competent musculature, the network described by the Hammock Hypothesis operates efficiently, favoring the maintenance of urinary continence throughout aging.
In an integrated manner, the results point to a multifactorial model in which postural alignment, muscle strength, perineal morphometry, and anthropometric characteristics interact to determine pelvic floor behavior. The interplay of these factors appears to be particularly relevant in aging populations, in which physiological changes associated with aging may exacerbate the vulnerability of the urethral support system. Thus, the findings contribute to improving the clinical understanding of pelvic floor dysfunctions, reinforcing the need for therapeutic approaches that integrate postural correction, muscle strengthening, and monitoring of modifiable factors, such as body mass index.
Among the limitations of this study, the cross-sectional design stands out, as it precludes the establishment of causal relations between the analyzed variables, restricting the interpretation of the findings to the identification of associations and limiting the precision of estimates, thereby increasing the risk of type I (false positive) and type II (false negative) errors. No specific corrections for multiple comparisons were applied, given the exploratory nature of the analysis; however, this choice should be considered when interpreting the results. Thus, the conclusions should be viewed as indications of association, reinforcing the need for cautious interpretation and for future investigations with larger samples and longitudinal designs to confirm the observed patterns. Furthermore, as this was an exploratory investigation aimed at analyzing relations between morphometric, clinical, and functional variables, no sample size calculation was performed. In addition, the small sample size and its recruitment within a specific context may limit the representativeness of the findings in relation to populations with different anthropometric, functional, and clinical characteristics. Therefore, although the observed patterns are biomechanically plausible and clinically coherent, they should be interpreted as preliminary evidence of association.
Although standardized methods for morphometric, postural, and perineometric assessment were used, the influence of inter-rater variability cannot be ruled out, nor can that of uncontrolled factors such as habitual physical activity level, parity, detailed obstetric history, and the presence of comorbidities, which may act as confounding factors.
Nevertheless, the observed patterns of interaction between postural alignment, pelvic morphometry, and pelvic floor function provide relevant conceptual support for understanding urethral support and urinary continence in clinical and preventive contexts, particularly in aging, and may guide hypotheses and future investigations across different settings and populations.
5. Conclusion
The findings of this study indicate that, in older women, morphometric measures of the pelvis and the lumbosacral region are significantly associated with factors predisposing to urinary incontinence. The interaction between structural support and pelvic floor functionality appears to be determinant for the maintenance of urinary continence, demonstrating that anatomical or postural changes may directly influence continence capacity. These results reinforce the importance of integrated physiotherapeutic assessments that consider both morphometric parameters and muscle contractile response, providing a basis for preventive strategies and clinical interventions focused on women’s pelvic health.
Despite the cross-sectional and exploratory nature of the study, which precludes causal inferences, the data provides valuable evidence on the patterns of association between pelvic morphology, lumbosacral alignment, and pelvic floor function, contributing to the planning of future research and targeted physiotherapeutic interventions.
AI use statement
The authors declare that artificial intelligence tools were used solely for language revision and stylistic suggestions during the writing process, without influencing data interpretation, hypothesis formulation, or any methodological decisions.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS e Scopus.
References
1. Grewar H, McLean L. The integrated
continence system: a manual therapy approach to the treatment of stress urinary
incontinence. Man Ther. 2008;13(5):375–86. https://doi.org/10.1016/j.math.2008.01.003
2. Kiapour A, Joukar A, Elgafy H, Erbulut DU, Agarwal AK, Goel VK. Biomechanics of the sacroiliac joint: anatomy, function, biomechanics, sexual dimorphism, and causes of pain. Int J Spine Surg. 2020;14(Suppl1):3-13. https://doi.org/10.14444/6077
3. Imai N, Suzuki H, Sakagami A, Hirano Y, Endo N. Correlation of the anatomical sacral slope with pelvic incidence in female patients with developmental hip dysplasia: a retrospective cross-sectional study. J Orthop Surg Res. 2020;15:486. https://doi.org/10.1186/s13018-020-02022-9
4. Brandão S, Parente M, Mascarenhas T,
Silva ARG, Ramos I, Jorge RN. Biomechanical study on the bladder neck and
urethral positions: simulation of impairment of the pelvic ligaments. J
Biomech. 2015;48(2):217-23. https://doi.org/10.1016/j.jbiomech.2014.11.045
5. Moreira SFS, Girão MJBC, Sartori MGF,
Baracat EC, Lima GR. Bladder Neck Mobility and Functional Pelvic Floor
Evaluation in Women with and without Stress Urinary Incontinence, According to
Hormonal Status. Rev Bras Ginecol Obstet. 2002;24(6):365-70. https://doi.org/10.1590/S0100-72032002000600002
6. DeLancey JOL. Structural support of the urethra as it relates to stress urinary incontinence: the hammock hypothesis. Am J Obstet Gynecol. 1994;170(6):1713-23. https://doi.org/10.1016/s0002-9378(94)70346-9
7. Ashton-Miller JA, DeLancey JOL. Functional Anatomy of the Female Pelvic Floor. Annals of the New York Academy of Sciences. 2007;1101:266-96. https://doi.org/10.1196/annals.1389.034
8. Bø K, Hilde G, Tennfjord MK, Sperstad JB, Engh ME. Pelvic floor muscle function, pelvic floor dysfunction and diastasis recti abdominis: Prospective cohort study. Neurourol Urodyn. 2017;36(3):716-21. https://doi.org/10.1002/nau.23005
9. Fielding JR. Practical MR imaging of female pelvic floor weakness. Radiographics. 2002;22(2):295-304. https://doi.org/10.1148/radiographics.22.2.g02mr25295
10. Pihl S, Uustal E, Blomberg M. Anovaginal distance and obstetric anal sphincter injury: a prospective observational study. Int Urogynecol J. 2019;30(6):939-44. https://doi.org/10.1007/s00192-018-3838-5
11. Megadhana IW, Marta KF, Arijaya DNK. Wide Genital
Hiatus (GH) and Short Perineal Body (PB) as Risk Factors for Stage III-IV
Uterine Prolapse. Eur J Med Health Sci. 2025;7(2):23-6. https://doi.org/10.24018/ejmed.2025.7.2.2257
12. Dancey CP, Reidy J. Statistics without
maths for psychology. 7th ed. Harlow: Pearson; 2017.
13. Subak LL, Richter HE, Hunskaar S. Obesity and urinary incontinence: epidemiology and clinical research implication. J. Urol. 2009;182(6 Suppl):S2-7. https://doi.org/10.1016/j.juro.2009.08.071
14. Whitcomb EL, Subak LL. Effect of
weight loss on urinary incontinence in women. Res Rep Urol. 2011;3:123-32. https://doi.org/10.2147/oaju.s21091
15. Dietz HP. Pelvic floor ultrasound: a review. Clin Obstet Gynecol. 2017;60(1):58-81. https://doi.org/10.1097/grf.0000000000000264
16. Swenson CW, Masteling M, DeLancey JO, Nandikanti L, Schmidt P, Chen L. Aging effects on pelvic floor support: a pilot study comparing young versus older nulliparous women. Int Urogynecol J. 2020;31(3):535-43. https://doi.org/10.1007/s00192-019-04063-z
17. Lemos AQ, Brasil CA, Alvares CM, Passos JCG, Lordêlo PP, Sá KN. The relation of the pelvis and the perineal function in incontinent women: a neglected subject. Neurourol Urodyn. 2018;37(8):2799-2809. https://doi.org/10.1002/nau.23772
18. Muellner M, Haffer H, Moser M, Chiapparelli E, Dodo Y, Amini DA, et al. Paraspinal musculature impairment is associated with spinopelvic and spinal malalignment in patients undergoing lumbar fusion surgery. Spine J. 2022;22(12):2006-16. https://doi.org/10.1016/j.spinee.2022.07.103
19. Hoyte L, Damaser M. Biomechanics of the female pelvic floor. 1st ed. London: Academic Press; 2016.
20. Reis AM, Brito LGO, Teixeira CPF, Araújo CC, Facio FA, Herrmann V, et al. Is There a Difference in Whole Body Standing Posture in Women With Urinary Incontinence Based on the Presence of Myofascial Dysfunction in the Pelvic Floor Muscles? Phys Ther. 2021;101(10):pzab171. https://doi.org/10.1093/ptj/pzab171
21. Capson AC, Nashed J, McLean L. The role of lumbopelvic posture in pelvic floor muscle activation in continent women. J Electromyogr Kinesiol. 2011;21(1):166-77. https://doi.org/10.1016/j.jelekin.2010.07.017
22. d'Aulignac D, Martins JAC, Pires EB, Mascarenhas T, Jorge RMN. A shell finite element model of the pelvic floor muscles. Comput Methods Biomech Biomed Engin. 2005;8(5):339-47. https://doi.org/10.1080/10255840500405378
