Case report
Effect of transcutaneous auricular vagal nerve stimulation associated with abdominal massage on constipation in an individual with type 2 diabetes with inadequate glycemic control: a case report / Efeito da estimulação transcutânea do nervo vago auricular associada à massagem abdominal na constipação em um indivíduo com diabetes tipo 2 e controle glicêmico inadequado: um relato de caso
Nijidha Manshi1. (https://orcid.org/0009-0001-2093-9459)
Vignesh Srinivasan2 (https://orcid.org/0000-0003-3378-4334)
Ahalya Sreekumaran3 (https://orcid.org/0009-0007-3958-4620)
Prathap Suganthirababu4 (https://orcid.org/0000-0002-1419-266X)
1,3,4Saveetha College of Physiotherapy, Saveetha Institute of Medical and Technical Sciences (SIMATS) (Chennai). Tamil Nadu, India.
2Corresponding contact. Saveetha College of Physiotherapy, Saveetha Institute of Medical and Technical Sciences (SIMATS) (Chennai). Tamil Nadu, India. [email protected]
ABSTRACT | INTRODUCTION: Constipation is common in people with untreated type 2
diabetes due to autonomic neuropathy and impaired vagal regulation of bowel
motility that negatively impacts their quality of life and general well-being.
Although abdominal massage is commonly used to support bowel movement, there is
little information on the utility of transcutaneous auricular vagal nerve
stimulation (taVNS) in diabetes constipation. However, the combined application
of these two non-invasive interventions in a single patient with inadequate
glycemic control has not been previously reported. This study explores the
effect of taVNS paired with abdominal massage in an individual with inadequate
glycemic control. OBJECTIVE:
This study aims to investigate the combined effect of taVNS and abdominal
massage on constipation in an individual with inadequate glycemic control in
type 2 diabetes mellitus. METHOD: A 50-year-old male with type 2
diabetes with inadequate glycemic control and persistent constipation requiring
regular laxative use underwent taVNS combined with abdominal massage for four
weeks. The taVNS was administered three times per week for 20 minutes (25 Hz,
25 mA), followed by 20 minutes of abdominal massage daily. Outcomes were
assessed using the Bristol Stool Scale (BSS) and the Patient Assessment of
Constipation Symptoms (PAC-SYM) questionnaire, with pre- and post- intervention
comparisons. RESULTS: The participant showed a decrease in PAC-SYM score
and stool consistency improved from Bristol type 2 to type 4. No adverse events
were observed during the intervention period. CONCLUSION: This case
report demonstrated that combined use of taVNS and abdominal massage may be
considered a supportive physiotherapy treatment for diabetes constipation.
KEYWORDS: Vagal Nerve Stimulation. Constipation. Diabetes Mellitus. Case Report.
RESUMO | INTRODUÇÃO: A constipação intestinal é comum em pessoas com diabetes tipo 2 não controlado, devido à neuropatia autonômica e à regulação vagal prejudicada da motilidade intestinal, o que impacta negativamente sua qualidade de vida e bem-estar geral. Embora a massagem abdominal seja comumente utilizada para auxiliar o funcionamento intestinal, há poucas informações sobre a utilidade da estimulação transcutânea do nervo vago auricular (taVNS) no tratamento da constipação em pacientes com diabetes. No entanto, a aplicação combinada dessas duas intervenções não invasivas em um único paciente com diabetes não controlado ainda não foi relatada. Este estudo explora o efeito da taVNS associada à massagem abdominal em um indivíduo com diabetes tipo 2 não controlado. OBJETIVO: Este estudo tem como objetivo investigar o efeito combinado da taVNS e da massagem abdominal na constipação em um indivíduo com diabetes mellitus tipo 2 não controlado. MÉTODO: Um paciente do sexo masculino, de 50 anos, com diabetes tipo 2, controle glicêmico inadequado e constipação persistente — que exigia o uso regular de laxantes —, foi submetido à taVNS combinada com massagem abdominal durante quatro semanas. A taVNS foi administrada três vezes por semana, por 20 minutos (25 Hz, 25 mA), seguida por 20 minutos de massagem abdominal diária. Os desfechos foram avaliados utilizando a Escala de Fezes de Bristol (BSS) e o Questionário de Avaliação de Sintomas da Constipação pelo Paciente (PAC-SYM), com comparações entre os períodos pré e pós-intervenção. RESULTADOS: O participante apresentou uma redução na pontuação PAC-SYM, e a consistência das fezes melhorou do tipo 2 para o tipo 4 na Escala de Fezes Bristol. Não foram observados eventos adversos durante o período de intervenção. CONCLUSÃO: Este relato de caso demonstrou que o uso combinado de taVNS e massagem abdominal pode ser considerado um tratamento fisioterapêutico complementar para a constipação em pacientes com diabetes.
PALAVRAS-CHAVE: Estimulação do Nervo Vago. Constipação. Diabetes Mellitus. Relato de Caso.
How to cite this article: Manshi N, Srinivasan V, Sreekumaran A, Suganthirababu P. Effect of transcutaneous auricular vagal nerve stimulation associated with abdominal massage on constipation in an individual with type 2 diabetes with inadequate glycemic control: a case report. J Physiother Res. 2026;16:e6670. https://doi.org/10.17267/2238-2704rpf.2026.e6670
Submitted Dec. 24, 2025, Accepted May 6, 2026, Published 10 July, 2026
J. Physiother. Res., Salvador, 2026;16:e6670
https://doi.org/10.17267/2238-2704rpf.2026.e6670
ISSN: 2238-2704
Assigned editor: Juliana Goulardins
1. Introduction
One of the major global health issues is diabetes, and one of the most common gastrointestinal symptoms of the disease is constipation1. Diabetic patients quality of life is affected by GI symptoms, which are common in diabetic autonomic neuropathy2. Many people experience physical and mental discomfort from constipation, which can seriously impair their everyday lives and general well-being3. Bowel motility is an important indicator of gastrointestinal health, and bowel sounds provide a non-invasive, real-time representation of intestinal peristaltic activity4.
The autonomic (parasympathetic and sympathetic) and enteric nerve systems interact to regulate the muscular, sensory, and secretory activities of the gastrointestinal (GI) tract. The gastrointestinal (GI) tract is innervated and significantly modulated by the vagal nerve. Vagal nerves, the tenth cranial nerves, are essential for controlling parasympathetic activity, which affects stomach motility and contributes to good health and well-being5. Long-term type 1 and type 2 diabetes are known to produce GI motility disorders, which are a major cause of morbidity and are commonly thought to be an indication of autonomic dysfunction. The autonomic nervous system uses sympathetic (mesenteric) and parasympathetic (vagal and pelvic) nerves to extrinsically modulate gut function6. Eighty percent of the vagal nerve's fibers are sensory (afferent), whereas twenty percent are motor (efferent)7.
A safe and comfortable technique that highlights the importance of the vagal nerve is transcutaneous auricular vagal nerve stimulation (taVNS)8. Recent evidence from randomized controlled trials has shown that vagal nerve stimulation, including transcutaneous auricular vagal nerve stimulation, can significantly improve bowel movement frequency and stool consistency in individuals with chronic constipation9. In addition, transcutaneous auricular vagal nerve stimulation has been reported to modulate autonomic function and promote physiological homeostasis, highlighting its potential as a non-invasive therapeutic approach10. Through mechanical stimulation of the colon, increased parasympathetic activity, and promotion of colonic transit, abdominal massage is a non-invasive intervention that may improve bowel motility and increase the frequency and consistency of stools. Previous literature suggests that abdominal massage may reduce constipation severity and improve bowel movement frequency and stool consistency across different populations11. Although each of these strategies has shown promising results when used alone, the existing evidence remains limited, and their combined effect has not been fully examined.
This case report focuses on an adult with type 2 diabetes, inadequate glycemic control and severe constipation. Due to persistent bowel dysfunction associated with autonomic involvement, the patient's gastrointestinal motility was impaired. However, there is currently limited information on the use of transcutaneous auricular vagal nerve stimulation along with abdominal massage in individuals with type 2 diabetes-related constipation. Additionally, there is a lack of preliminary clinical data examining this combined approach, particularly in individuals with poor glycemic control. To the best of our knowledge, very few studies have examined transcutaneous auricular vagal nerve stimulation in constipation associated with type 2 diabetes, and none have particularly examined its use in conjunction with abdominal massage in this population. Therefore, a case report was thought to be a suitable first step in examining the viability and possible outcomes of this combination intervention. This case report aims to describe the application of transcutaneous auricular vagal nerve stimulation combined with abdominal massage for constipation in an individual with type 2 diabetes with inadequate glycemic control. Since physiotherapy techniques focus on autonomic regulation and intestinal motility, this study may help with clinical decision-making for the physiotherapeutic treatment of diabetes constipation.
2. Method
In this single case report, the effect of abdominal massage and transcutaneous auricular vagal nerve stimulation (taVNS) on constipation in an individual with type 2 diabetes mellitus characterized by inadequate glycemic control was evaluated. Approval was obtained from the Institutional Scientific Review Board before participant recruitment (027/05/2025/ISRB/PGSR/SCPT). Prior to participation, written informed consent was obtained. The participant was a 50-year-old male with type 2 diabetes mellitus, exhibiting chronic constipation that requires frequent usage of laxatives. The participant was selected based on the presence of persistent constipation lasting longer than three months, a diagnosis of type 2 diabetes mellitus with inadequate glycemic control (HbA1c >7%), and a regular dependence on laxatives. The case was selected because it is clinically reasonable to look at non-pharmacological treatments targeting autonomic dysfunction when inadequate glycemic control and chronic constipation coexist. The Bristol Stool Scale was used to quantify stool consistency, and the Patient Assessment of Constipation Symptoms (PAC-SYM) Questionnaire was used to assess the intensity of symptoms. The subject was observed for any adverse events during and after each session. Pre- and post-intervention scores were recorded and compared to determine the clinical improvement. Because of the single-case design, a descriptive technique was used to analyze the data, comparing scores before and after the intervention to assess changes in clinical outcomes. In order to ensure thoroughness and transparency in clinical case reporting, this case report was written and reported in compliance with the CARE Guidelines.
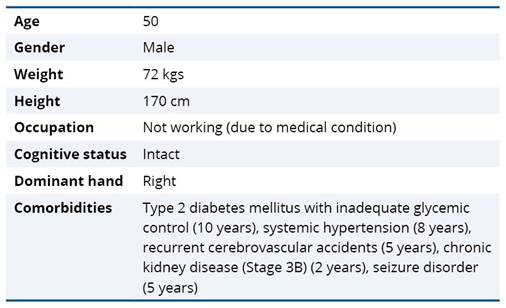
2.1 Patient Information
A 50-year-old male, known case of recurrent cerebrovascular accidents, seizure disorder, chronic kidney disease stage 3B, type 2 diabetes mellitus with inadequate glycemic control, systemic hypertension, presented with complaints of vomiting and loose stools for 3 days. His attender reported a history of chronic constipation for the past 1.5 years, requiring regular use of laxatives. There was no relevant family history of digestive or metabolic problems. During the intervention period, the participant's medication use, hydration levels, and dietary habits (including fiber intake) were assessed. The use of laxatives stayed constant during the study period, and no significant changes in food, fluid intake, or prescribed medications were noted. The individuals’ ongoing gastrointestinal problems significantly affected their daily comfort and quality of life. All assessments and interventions were conducted in an inpatient setting, and the individual stayed in the hospital throughout the intervention.
Table 1. Demographic data of participant
2.2 Clinical findings
On physical examination, the patient was conscious and oriented. Examining the abdomen revealed slow bowel movements. Neurological findings showed motor aphasia, upper limb muscle power 4/5, and lower limb muscle power 3/5. These findings suggested that the participants underlying neurological and metabolic disorders were linked to decreased neuromuscular function.
2.3 Diagnostic assessment
In order to evaluate intestinal function and support the diagnosis of constipation, a diagnostic evaluation was conducted. The results of the abdominal computed tomography report, which showed fecal loading in the rectum with noticeable bowel loops, were consistent with constipation. The Bristol Stool Scale was used to measure stool consistency, and the Patient Assessment of Constipation Symptoms (PAC-SYM) questionnaire was used to evaluate the intensity of constipation symptoms. These standardized tools were used to record gastrointestinal function at baseline and at follow-up. Laboratory tests revealed glycated hemoglobin (HbA1c) values above 7%, a sign of poor glycemic control in type 2 diabetes. Based on the clinical history and imaging results, other possible causes of constipation, such as medication-induced constipation and mechanical intestinal blockage, were taken into consideration and ruled out. This result supported that constipation, autonomic dysfunction, and prolonged hyperglycemia were related in this case.
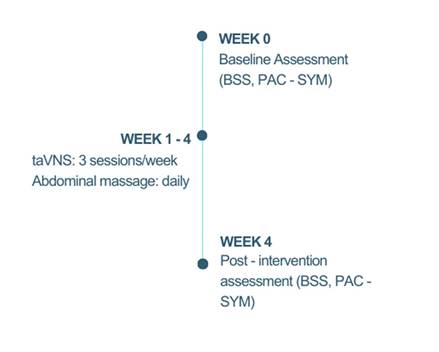
2.4 Timeline
Baseline stool consistency and gastrointestinal symptoms were assessed using the Bristol Stool Scale (BSS) and Patient Assessment of Constipation Symptoms (PAC-SYM) questionnaire at week 0 after the clinical evaluation. Following that, the participant underwent three sessions of transcutaneous auricular vagal nerve stimulation (taVNS) and daily abdominal massages for four consecutive weeks (weeks 1-4). Using the same outcome measures, a post-intervention assessment was carried out at the end of week four. Figure 1 shows the timeline for the intervention.
Figure 1. Timeline of intervention and assessment protocol
2.5 Therapeutic intervention
Abdominal massage and transcutaneous auricular vagal nerve stimulation (taVNS) were used in a combination non-pharmacological physiotherapy strategy to enhance bowel movement. Transcutaneous auricular vagal nerve stimulation (taVNS) was administered using clip electrodes placed on the cymba concha of the left ear, targeting the auricular branch of the vagal nerve, using a commercially available interferential therapy device (IFT Combo Therapy 4 in 1, DE Group of Delta, India) with ear clip electrodes (ELBME®, ear clip type electrode leads; wire length approximately 3.9 ft; plug diameter 0.09 inch). The stimulation was delivered for 20 minutes with the following parameters: a frequency of 25 Hz and a pulse width of 330 μs. The stimulation intensity was adjusted based on the participant's sensory threshold and maintained at 25 mA, ensuring a strong but tolerable sensation below the pain threshold. The intervention was administered three times a week for a duration of four weeks. According to earlier studies, the stimulation intensity in transcutaneous auricular vagal nerve stimulation (taVNS) is often tailored according to sensory experience and can vary depending on the anatomical region of stimulation, electrode characteristics, and skin impedance. In order to achieve adequate neural activation, transcutaneous applications may need higher current intensities due to the resistance of the skin and superficial tissues. The use of up to 25 mA in this case constitutes patient-specific titration to the highest acceptable, painless level in compliance with methodological standards that prioritize tailored dosage over predefined intensity limits12. Immediately following taVNS, the participant received abdominal massage for 20 minutes, consisting of gentle, circular, clockwise strokes along the course of colon to facilitate bowel motility. The massage was administered by a trained physiotherapist and followed the colon's anatomical course (ascending, transverse, descending, and sigmoid colon). The taVNS sessions were administered three times per week, and abdominal massage was performed daily for four consecutive weeks. This frequency was selected based on prior evidence that intermittent taVNS (2-3 sessions per week) is sufficient to induce sustained autonomic effects, while daily abdominal massage provides continuous mechanical facilitation of bowel motility and enhance therapeutic consistency. The intervention protocol was not altered while the patient was receiving treatment. All sessions were well tolerated by the individual, and no negative events were noted.
2.6 Follow up and outcomes
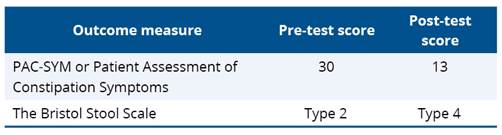
Outcome measures were recorded at baseline prior to the intervention and reassessed at the end of the four-week intervention. After four weeks of intervention pre- and post- intervention showed improvement in bowel function. From type 2 to type 4, the Bristol Stool Scale (BSS) score increased, suggesting a change toward normal stool consistency. The PAC-SYM score also showed a decrease in constipation severity, from 30 to 13. Detailed pre- and post-intervention scores are provided in Table 2. No adverse events occurred during the intervention period, and the participant completed all scheduled sessions. Tolerability was evaluated through patient self-report and observation during each session, and adherence was tracked by attendance at all scheduled sessions.
Table 2. Pre and Post test scores using the Bristol Stool Scale and the Patient Assessment of Constipation Symptoms (PAC-SYM)
3. Discussion
Following the four-week intervention, the participant's constipation-related outcomes improved. The PAC-SYM score decreased from 30 to 13 (absolute change of -17 points, corresponding to a 56.7% reduction) after the four-week intervention, indicating a considerable improvement in the frequency of bowel movements and a decrease in discomfort associated with constipation. The use of laxatives did not change during the intervention period, contributing to overall well-being. Stool consistency also improved from Bristol type 2 to type 4, according to the assessment carried out at the end of the four-week intervention period. The positive response suggests that the diabetic patient's intestinal motility may have been enhanced by the combination of taVNS and abdominal massage. Although the observed improvement suggests a potential connection between the intervention and the outcomes, causal inferences cannot be made due to the single-case methodology.
Recent findings from a meta-analysis and comprehensive review of randomized controlled trials indicate that vagal nerve stimulation is a useful treatment for chronic constipation. After vagal neuromodulation, the evaluation showed notable changes in bowel movement frequency, stool consistency, and constipation-related symptoms. 9 These findings are consistent with the current case, where transcutaneous auricular vagal nerve stimulation combined with abdominal massage resulted in higher Bristol Stool Scale scores and lower PAC-SYM scores. This findings further supports the potential of vagal neuromodulation as a non-pharmacological method to reduce constipation symptoms and improve gastrointestinal motility. Data from a recent narrative review indicates that abdominal massage may effectively improve the regularity and consistency of bowel movements across a range of demographics and reduce the severity of constipation11. These results align with the current instance, in which daily massage of the abdomen improved bowel function.
Song et al. highlighted the potential of transcutaneous electrical stimulation as a safe, noninvasive, and home-based method for managing gastrointestinal motility disorders13. Similarly, the present case supports this finding, showing that taVNS combined with abdominal massage may enhance bowel motility and relieve constipation through autonomic modulation. Kornum et al. found that cervical taVNS did not improve gastrointestinal symptoms in diabetic autonomic neuropathy14. However, the present case showed improvement with auricular taVNS and abdominal massage, suggesting that the auricular approach, combined with mechanical stimulation, may be more effective for enhancing bowel motility in diabetic constipation. In a study by Gottfried-Blackmore et al., patients with idiopathic gastroparesis experienced improved symptoms and faster stomach emptying after receiving short-term non-invasive vagal nerve stimulation, with greater benefits observed in those with more severe baseline delays15. Similarly, the present case demonstrated improvement in gastrointestinal function following auricular taVNS combined with abdominal massage, suggesting that vagal modulation may enhance gut motility and symptom relief. These findings suggest that vagal stimulation may play a part in the treatment of gastrointestinal disorders, particularly in individuals with diabetes-related constipation. Although previous studies have evaluated transcutaneous auricular vagal nerve stimulation and abdominal massage as individual therapy, there is limited information on their combined use. Therefore, the current case explores their combined effect on the autonomic and mechanical regulation of bowel function in an individual with type 2 diabetes mellitus characterized by inadequate glycemic control. This combined method may offer a more thorough physiotherapy treatment for constipation in patients with diabetes, although it has not received much attention in the literature yet.
The present case report suggests that transcutaneous auricular vagal nerve stimulation combined with abdominal massage may effectively improve bowel movement and reduce constipation symptoms in an individual with type 2 diabetes mellitus characterized by inadequate glycemic control. This observed benefit could be explained by the combined mechanical and autonomic effects of the intervention. The introduction of a multimodal, non-pharmacological physiotherapy intervention evaluated using validated outcome measures is a major strength of this case report.
As this study involves a single case with a short duration of intervention, the results cannot be generalized. The results should be carefully considered because a single-case design makes it impossible to establish a causal relationship between the intervention and the observed outcomes. In addition, the individual effects of transcutaneous auricular vagal nerve stimulation and abdominal massage cannot be differentiated because both therapies were given concurrently during the study period. Confounding variables that were not controlled, such as medication use, food habits, hydration levels, and other coexisting conditions, may also have affected the outcomes. Additionally, the impact of the inpatient hospital setting which includes supervised care and structured routines as well as the potential for a placebo effect could have contributed to the noted benefits. However, the positive outcome suggests that this combined approach may serve as a potentially safe, non-invasive, adjunct in managing diabetic constipation. Further studies with larger sample sizes and extended intervention periods are recommended to substantiate these findings.
These findings might only be relevant to individuals with similar clinical characteristics, such as persistent constipation and type 2 diabetes with inadequate glycemic control and autonomic dysfunction. The observed results cannot be generalized beyond this context due to the inherent methodological limitations of a single-case study. More research, including case series and randomized controlled clinical trials, is required to validate these findings and establish clearer clinical criteria for their application. To further evaluate and strengthen the practical application of these findings, future research may also incorporate pilot studies and investigations using objective autonomic and gastrointestinal outcome markers. Methodological and ethical concerns must also be carefully taken into account when extrapolating these results to wider populations.
3.1 Patient perspective
The patient reported greater comfort, less straining during defecation, and voiced satisfaction with the therapy process. The participant expressed satisfaction with the combined intervention and noted that, if needed, they would be open to continuing to use such non-pharmacological treatments.
4. Conclusion
This study suggests that abdominal massage plus transcutaneous auricular vagal nerve stimulation may be associated with improvements in bowel function and reduced constipation symptoms in a person with type 2 diabetes with inadequate glycemic control. The improvement observed may be due to modulation of vagal activity and stimulation of intestinal motility. Although limited to a single case, the findings suggest that this combined, non-invasive approach holds promise as a supportive physiotherapy intervention for managing diabetic constipation.
AI disclosure statement
The authors used ChatGPT (OpenAI) to assist with grammar corrections and language improvement during the manuscript editing stage. Artificial intelligence tools were not used in the data creation, processing, or interpretation processes. All content was assessed, verified, and approved by the authors, who take all responsibility for the work's accuracy and integrity.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Abdu Seid M, Diress M, Mohammed A, Sinamaw D. Chronic constipation and its associated factors in patients with type-2 diabetes: a multicenter cross-sectional study. Diabetes Res Clin Pract. 2023;204:110905. https://doi.org/10.1016/j.diabres.2023.110905
2. Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U, Shaw JE. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res Clin Pract. 2014;103(2):137-49. https://doi.org/10.1016/j.diabres.2013.11.002
3. Mogess WN, Mihretie TB, Habte ML, Feyisa TO, Areda BG, Ahmed ET, et al. The magnitude of chronic constipation and associated factors among type 2 diabetic patients in Harar, Eastern Ethiopia. Clin Diabetes Endocrinol. 2024;10(1):33. https://doi.org/10.1186/s40842-024-00188-3
4. Wang G, Wang M, Liu H, Zhao S, Liu L, Wang W. Changes in bowel sounds of inpatients undergoing general anesthesia. Biomed Eng Online. 2020;19(1):60. https://doi.org/10.1186/s12938-020-00805-z
5. Liu J, Lv C, Yin M, Zhu M, Wang B, Tian J, et al. Efficacy and safety of transcutaneous auricular vagus nerve stimulation in patients with constipation-predominant irritable bowel syndrome: a single-center, single-blind, randomized controlled trial. Am J Gastroenterol. 2025;120(9):2139-53. https://doi.org/10.14309/ajg.0000000000003257
6. Phillips LK, Rayner CK, Jones KL, Horowitz M. An update on autonomic neuropathy affecting the gastrointestinal tract. Curr Diab Rep. 2006;6(6):417-23. https://doi.org/10.1007/s11892-006-0073-0
7. Ruthubalan V, Srinivasan V, Suganthirababu P, Abathsagayam K. Technological advancements in the treatment of anxiety and quality of sleep among teaching professionals: a pilot study. Res J Pharm Technol. 2025;18(1):333-8. https://doi.org/10.52711/0974-360X.2025.00052
8. Srinivasan V, Ruthuvalan V, Raja S, Jayaraj V, Sridhar S, Kothandaraman M, et al. Efficacy of vagal nerve stimulation on anxiety among elderly retired teachers during the COVID-19 pandemic. Work. 2024;79(2):645-52. Cited: PMID: 38489208
9. Saleh AO, Awashra A, Abouelmagd AA, Elkholy M, Hasanin EH, Aldohni AAA, et al. Vagal nerve stimulation for chronic constipation: a systematic review and meta-analysis of randomized controlled trials. Neuromodulation. 2026;S1094715926000103. https://doi.org/10.1016/j.neurom.2026.01.005
10. Sakthi R, Srinivasan V, Suganthirababu P, Kumar P, Dhanusia S, Kumaresan A, et al. Effect of vagal nerve stimulation on anxiety and sleep disturbances among geriatric population: a pilot study. Indian J Physiother Occup Ther. 2024;18:145-50. https://doi.org/10.37506/0cyxte86
11. Durga G, Mooventhan A, Gowthami R, Nivethitha L, Manavalan N. Scientific evidence-based effects of abdominal massage in people with constipation: a narrative review. Int J Ther Massage Bodywork. 2025;18(4):76-84. https://doi.org/10.3822/ijtmb.v18i4.1137
12. Olsen LK, Solis E, McIntire LK, Hatcher-Solis CN. Vagus nerve stimulation: mechanisms and factors involved in memory enhancement. Front Hum Neurosci. 2023;17:1152064. https://doi.org/10.3389/fnhum.2023.1152064
13. Song G, Trujillo S, Fu Y, Shibi F, Chen J, Fass R. Transcutaneous electrical stimulation for gastrointestinal motility disorders. Neurogastroenterol Motil. 2023;35(11):e14618. https://doi.org/10.1111/nmo.14618
14. Kornum DS, Bertoli D, Kufaishi H, Wegeberg AM, Okdahl T, Mark EB, et al. Transcutaneous vagal nerve stimulation for treating gastrointestinal symptoms in individuals with diabetes: a randomized, double-blind, sham-controlled, multicentre trial. Diabetologia. 2024;67(6):1122-37. https://doi.org/10.1007/s00125-024-06129-0
15. Gottfried-Blackmore A, Adler EP, Fernandez-Becker N, Clarke J, Habtezion A, Nguyen L. Open-label pilot study: non-invasive vagal nerve stimulation improves symptoms and gastric emptying in patients with idiopathic gastroparesis. Neurogastroenterol Motil. 2020;32(4):e13769. https://doi.org/10.1111/nmo.13769
