Original article
Effect of kinesio taping combined with myofascial release on hamstring spasticity in children with spastic diplegic cerebral palsy: a pilot randomized controlled trial / Efeito do kinesio taping combinado com liberação miofascial na espasticidade dos isquiotibiais em crianças com paralisia cerebral espástica diplégica: um ensaio randomizado controlado piloto
Pragati Singh Chauhan1 (https://orcid.org/0009-0006-6032-9790)
Adarsh Kumar Srivastav2 (https://orcid.org/0000-0002-6808-0401)
1Chhatrapati Shahu Ji Maharaj University (Kanpur). Uttar Pradesh, India.
2Corresponding contact. Chhatrapati Shahu Ji Maharaj University (Kanpur). Uttar Pradesh, India. [email protected]
ABSTRACT | INTRODUCTION: Hamstring spasticity in children with spastic diplegic cerebral palsy (CP) contributes to knee flexion deformity and functional limitations. Evidence regarding the combined effect of kinesio taping (KT) and Myofascial Release (MFR) remains limited. AIM: To investigate the adjuvant effect of KT combined with MFR on hamstring spasticity. METHODS: A two-group pre–post pilot randomized controlled trial was conducted. Twenty-six participants were randomized; twenty completed the study (10 per group). Both groups received 60 minute therapy sessions, three times per week for two weeks. The experimental group received 10 minutes of myofascial release followed by kinesio taping and conventional therapy, while the control group received conventional therapy alone. Outcomes (MAS and knee ROM) were assessed pre-and post-intervention. Data were analysed using appropriate parametric/non parametric tests after a normality check (Shapiro–Wilk test), with the significance level set at p < 0.05. RESULTS: Both groups demonstrated significant within-group improvements in MAS and ROM (p < 0.05). No significant between-group differences were observed (p > 0.05). CONCLUSION: The combined intervention demonstrated short-term within-group improvements but did not show superiority over conventional physiotherapy. Larger trials are required.
KEYWORDS: Cerebral Palsy. Spastic. Physical Therapy Modalities. Athletic Tape. Myofascial Release Therapy. Randomized Controlled Trial.
TRIAL REGISTRATION: CTRI/2025/04/084469, Registered 9 April 2025, CTRI.
RESUMO | INTRODUÇÃO: A espasticidade dos isquiotibiais em crianças com paralisia cerebral espástica diplégica contribui para a deformidade em flexão do joelho e limitações funcionais. As evidências sobre o efeito combinado do kinesio taping (KT) e da liberação miofascial (LMF) ainda são limitadas. OBJETIVO: Investigar o efeito adjuvante do KT combinado com LMF na espasticidade dos isquiotibiais. MÉTODOS: Foi realizado um ensaio clínico piloto randomizado pré–pós em dois grupos. Vinte e seis participantes foram randomizados; vinte completaram o estudo (10 por grupo). Ambos os grupos receberam sessões de terapia de 60 minutos, três vezes por semana durante duas semanas. O grupo experimental recebeu 10 minutos de liberação miofascial seguidos de kinesio taping e terapia convencional, enquanto o grupo controle recebeu apenas a terapia convencional. Os desfechos (Escala de Ashworth Modificada [MAS] e amplitude de movimento do joelho) foram avaliados antes e após a intervenção. Os dados foram analisados usando testes paramétricos/não paramétricos apropriados após a verificação de normalidade (teste de Shapiro–Wilk), com o nível de significância estabelecido em p < 0,05. RESULTADOS: Ambos os grupos demonstraram melhorias significativas intragrupo em MAS e ADM (p < 0,05). Nenhuma diferença significativa entre os grupos foi observada (p > 0,05). CONCLUSÃO: A intervenção combinada demonstrou melhorias de curto prazo intragrupo, mas não mostrou superioridade em relação à fisioterapia convencional. Ensaios maiores são necessários.
PALAVRAS-CHAVE: Paralisia Cerebral. Espástico. Modalidades de Fisioterapia. Fita Atlética. Terapia de Liberação Miofascial. Ensaio Clínico Randomizado.
REGISTRO DO ENSAIO: CTRI/2025/04/084469, Registrado em 9 de abril de 2025, CTRI.
How to cite this article: Chauhan PS, Srivastav AK. Effect of kinesio taping combined with myofascial release on hamstring spasticity in children with spastic diplegic cerebral palsy: a pilot randomized controlled trial. J Physiother Res. 2026;16:e6598. https://doi.org/10.17267/2238-2704rpf.2026.e6598
Submitted Nov. 21, 2025, Accepted Apr. 9, 2026, Published May 28, 2026
J. Physiother. Res., Salvador, 2026;16:e6598
https://doi.org/10.17267/2238-2704rpf.2026.e6598
ISSN: 2238-2704
Assigned editor: Juliana Goulardins
1. Introduction
Cerebral palsy is a prevalent movement and posture disorder causing physical disability among children1. Cerebral palsy is caused by permanent damage to the developing immature brain before birth, at the time of birth, or just after birth2.
Worldwide, the prevalence of cerebral palsy is 2.4 per 1000 children aged 3 to 10 years, while the incidence rate is 2 to 3 per 1000 live births2,3. Primary neuromuscular impairments, including spasticity, muscle weakness, and decreased selective motor control, as well as musculoskeletal problems, such as bony deformities and contractures, are characteristics of cerebral palsy4. MRI scan abnormalities and motor dysfunctions are used to identify cerebral palsy1,5. Depending on the kind of movement impacted, the body parts involved, and the area of the brain damaged, the primary forms of cerebral palsy are spastic, dyskinetic, ataxic, and mixed1,6.
Spastic diplegia is the most common type of CP, accounting for 35 percent of children with CP, and is characterised by stiff, tight muscles due to increased muscle tone7. In diplegics, lower extremities are more spastic than the upper extremities8,9. Spastic diplegics usually have increased muscle tone in adductors, calves, and the hamstring muscle groups10. Symptoms include fatigue, muscle shortness, reduced range of joint mobility, contractures, and joint subluxations7.
Over the years, CP has been managed using a variety of approaches, including acupuncture, neurodevelopmental training, sensory integration, electrical stimulation, hippotherapy, music therapy, and stretching11–13. One of the recent treatments is the application of kinesio taping (KT), which, in combination with other physiotherapy interventions, has been chosen for better results in this category of patients9,14. A therapeutic tape called kinesio tape aids in supporting and easing joint, ligament, and muscle pain9,14. The elasticity of kinesio tape lifts and tightens the skin from soft tissues when it is placed effectively13,15–17.
Myofascial release (MFR) is a contemporary technique aimed at releasing tension within myofascial tissues to alleviate pain and improve movement18. MFR techniques involve gentle stretching and compressing of the fascia to target restrictions, improve mobility, and reduce pain18. The MFR technique has produced consistent results in children with cerebral palsy suffering from spasticity19.
Beyond its clinical implications, identifying effective, low-cost, and accessible interventions for spastic diplegic cerebral palsy holds significant social and economic importance, particularly in resource-limited settings. Strategies that improve mobility may enhance participation and reduce caregiver burden, while cost-effective, non-invasive techniques may lessen long-term financial strain. Furthermore, conducting a randomized controlled trial to evaluate the combined effect of myofascial release and kinesiology taping addresses an existing methodological gap in pediatric neurorehabilitation literature. This pilot randomized controlled trial aimed to evaluate the short-term adjuvant effect of KT combined with MFR on hamstring spasticity.
2. Methodology
2.1 Study design
A two-group pre-post pilot randomized controlled trial approved by the Institutional Ethics Committee, School of Health Sciences, Chhatrapati Shahu Ji Maharaj University (Kanpur) (HEC Reference Number: 2024-Jun-010). The study was registered with the Clinical Trials Registry of India(CTRI); CTRI/2025/04/084469 (CTRI). The study location was the School of Health Sciences, Chhatrapati Shahu Ji Maharaj University, Kanpur, Uttar Pradesh.
2.2 Participant recruitment and allocation
The inclusion criteria included: both male and female diagnosed with spastic diplegic CP; age group 4-12 years; spasticity grades 1, 1+, 2, and 3 as per the Modified Ashworth Scale on hamstrings; ambulatory children with or without ambulatory devices. The exclusion criteria included: skin sensitivity; other types of cerebral palsy; Botox injection if taken in the past six months; knee flexion contracture; and any prior orthopaedic surgery8,20.
2.3 Sampling method and sample size
The sampling method used was purposive sampling. The sample size was calculated using G*Power 3.1.9.7 software with an alpha level of 0.05, a beta level of 0.80, and an effect size of 1.358,20. Considering a 30% dropout rate in the study, 26 participants were recruited.
2.4 Randomization
Using a standard computerized tool (computer-generated random sequence via randomizer.org; http://www.randomizer.org/index.htm), children were randomly divided into the experimental and control groups after their parents provided written informed consent. The allocation sequence was generated by an independent researcher who was not involved in participant recruitment or assessment. Allocation concealment was ensured using sealed, opaque envelopes to prevent selection bias. Both the development of the unbiased allocation sequence and the process of allocation concealment were maintained in compliance with the Consolidated Standards of Reporting Trials (CONSORT) statement. The materials used in the study included kinesio tape, scissors, gel, floor mats, a stool, a gym ball, and a goniometer20.
2.5 Outcome measures
The outcome measures used were the Modified Ashworth Scale (MAS) and Range of Motion (ROM)8,20–23. The Modified Ashworth Scale was selected as the primary outcome measure for spasticity assessment due to its widespread clinical acceptance, easy administration, and good intrarater reliability 0.84 and good interrater reliability 0.8320. Goniometry is used as a quantitative measurement tool in this study20. The intratester and intertester reliability coefficients of goniometric measurement of knee joint flexion are 0.90 and 0.86, respectively, according to ICC (Intraclass Correlation Coefficient)20.
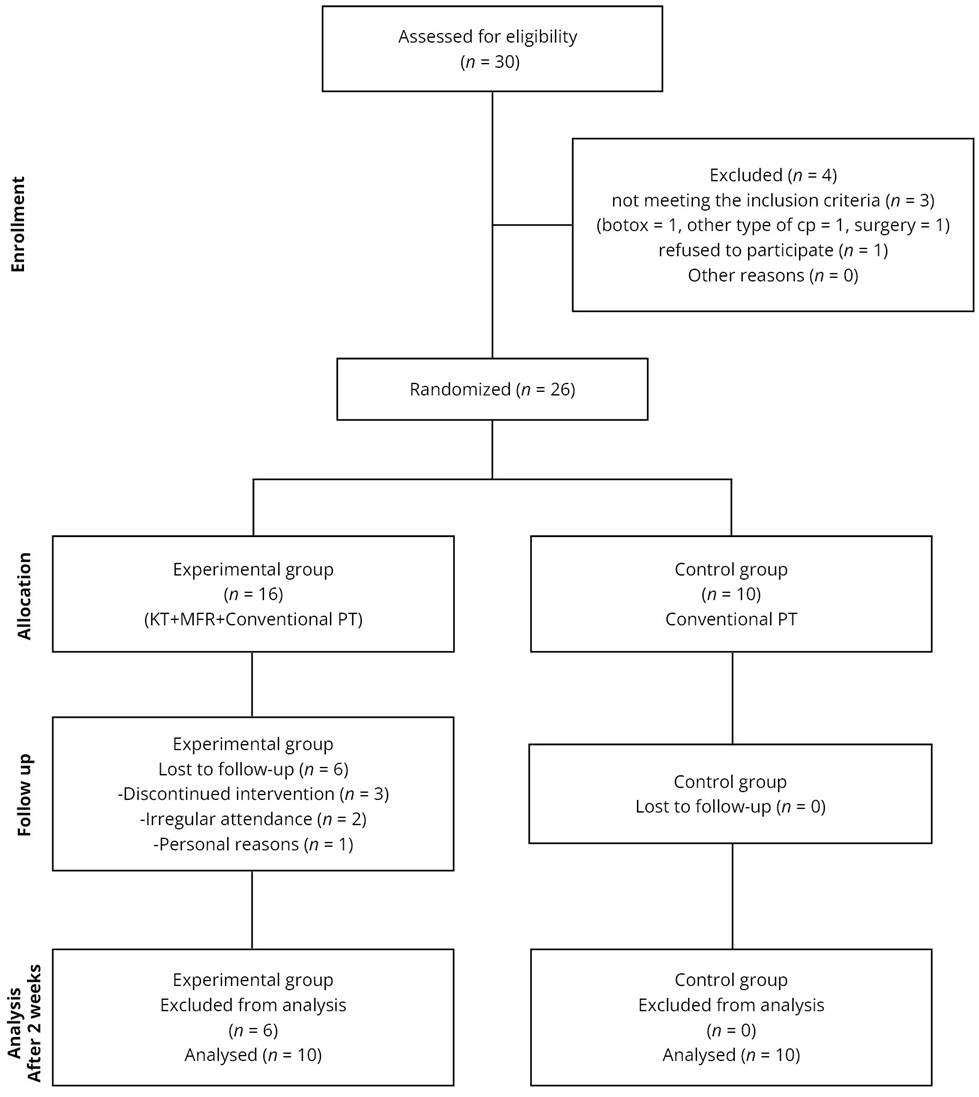
Figure 1. CONSORT Flowchart of the participants
2.6 Procedures
Step 1: Every participant from the approved data source was evaluated, and those who met the inclusion criteria were recruited.
Step 2: Using a computer-generated randomization method, all individuals were divided into two groups:
• Group A: Conventional physiotherapy, myofascial release, and Kinesio taping;
• Group B: Conventional physiotherapy treatment only.
Step 3: All children’s parents were informed about the entire procedure, and their signed informed consent was obtained.
Step 4: Before and after the intervention, all subjects were assessed using the Modified Ashworth Scale (MAS) for the hamstring muscle in the prone position.
Step 5: Intervention:
Both groups received 60-minute sessions, three times per week for two weeks.
• Experimental group (Group A): Received 10 minutes of myofascial release (MFR) with kinesio taping (KT) application, followed by conventional physiotherapy;
• Control group (Group B): Received conventional physiotherapy only.
Group A: Experimental group
Protocol for myofascial release (MFR):
Myofascial structures were stretched and held for 120 seconds while the patient was in the prone position, with the therapist’s hands or thumbs crossed, allowing the tissue to soften. The procedure was conducted for a total duration of 10 minutes19.
Figure 2. Myofascial release on hamstrings

Protocol for kinesio taping:
Taping was applied to the hamstring muscles to inhibit knee flexion. For inhibitory actions, it was applied from the end toward the beginning of the muscle (insertion to origin). An I-shaped strip was applied over the muscle belly. The tension of the tape in the muscular area was set at 30% of its original length8. Following MFR and kinesio taping, all individuals received the same standard physical therapy treatment as the control group, three alternate days per week for 2 weeks.
Figure 3. Kinesio taping on hamstrings

Group B: Control Group
Conventional physiotherapy treatment:
Children in the control group continued with passive stretching of hamstrings (10 second hold, 5 repetitions, 2 sets); weight-bearing exercises (10 repetitions); bridging (bilateral and unilateral), kneeling, sit-to-stand, one-leg standing, mini squats, and stepping (forward, backward, and sideways)-10 repetitions each, 2 sets; gait training using parallel bars (10 repetitions). There was no subdivision of time for each activity and no specific time allocation for any task.
Step 6: At the end of the second week, the effect of the intervention was assessed using MAS and a goniometer. Data for MAS were recorded and analysed using an appropriate statistical test.
2.7 Data analysis
The collected data were analysed using IBM SPSS Statistics version 26.0.0. Normality was tested with the Shapiro-Wilk test, as the sample size was less than 50. Of the outcomes, seven were normally distributed, while nine did not show a normal distribution. Statistical analysis was performed using the parametric tests (for normally distributed data), i.e., the Paired- t test for within-group analysis and Independent- t test for between-group analysis, respectively; and non-parametric tests (for non-normally distributed data), i.e., the Wilcoxon Signed Rank test for within-group analysis and Mann-Whitney U test for between-group analysis, respectively. The level of significance was set at p-value <0.05. The demographic data were presented as mean(±SD), median (IQR), range, and p-value. The baseline characteristics of outcomes were expressed in terms of mean with 95%CI, median with range, and standard deviation. For primary and secondary outcomes within-group comparisons, results were expressed as mean and median with IQR for pre-and post-intervention values, along with p-values. The analysis of primary and secondary outcome measures was reported as median with range and p-value. The Post hoc power analysis was performed using G*Power 3.1.9.7, based on Cohen’s d effect sizes presented in tables 4, 5, 6, and 7. Cohen’s d effect sizes were calculated using pooled standard deviations for between-group comparisons. Achieved power (1−β) was computed using alpha = 0.05. Effect sizes were interpreted as small (0.2), medium (0.5), and large (≥0.8).
3. Results
Twenty-six participants were randomized, and twenty completed the study (10 per group). Six participants from the experimental group were lost to follow-up due to discontinuation or irregular attendance. Baseline demographic and clinical characteristics were comparable between groups. The demographics of participants and group distribution are depicted in Table 1, and the gender distribution of patients is depicted in Table 2. The baseline characteristics of study participants are presented in Table 3. The mean age of participants was 5.85 years (Standard Deviation was 1.80). Thirteen participants were male, and seven were female. Significant within-group improvements were observed in both groups for MAS and ROM (p < 0.05). However, no statistically significant between-group differences were found (p > 0.05), as shown in Tables 4, 5, 6, and 7. Effect size analysis demonstrated negligible-to-small effects for most MAS variables (d = 0–0.33), with a moderate effect observed for right knee extension (d = 0.69). ROM variables showed small-to-moderate effects (d = 0.14–0.69), particularly for the knee lacking extension. Post hoc power analysis indicated insufficient power for most MAS variables (≤0.50). Adequate power (>0.80) was observed only for the right knee lacking extension.
Table 1. Demographic characteristics of study participants (N = 20)
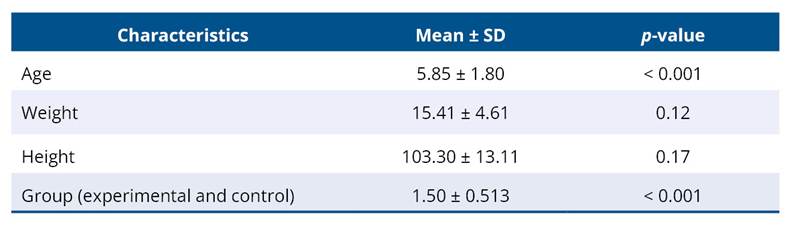
Table 2. The frequency and percentage of the gender distribution

Table 3. Baseline characteristics of study participants
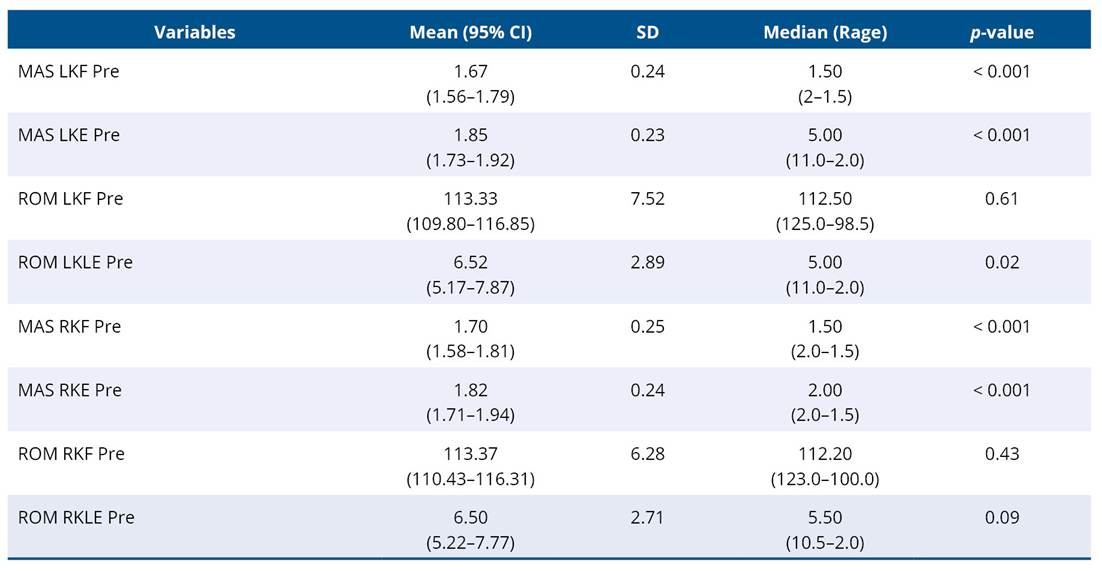
Abbreviations: SD -
Standard Deviation, MAS - Modified Ashworth Scale, LKF - Left Knee Flexion, LKE
- Left Knee Extension, ROM - Range of Motion,
LKLE - Left Knee Lacking Extension, RKF - Right Knee Flexion, RKE - Right Knee
Extension, RKLE -Right Knee Lacking Extension.
Note: p-value less than 0.05 shows significance.
Table 4. Within-group changes in Modified Ashworth Scale (MAS)
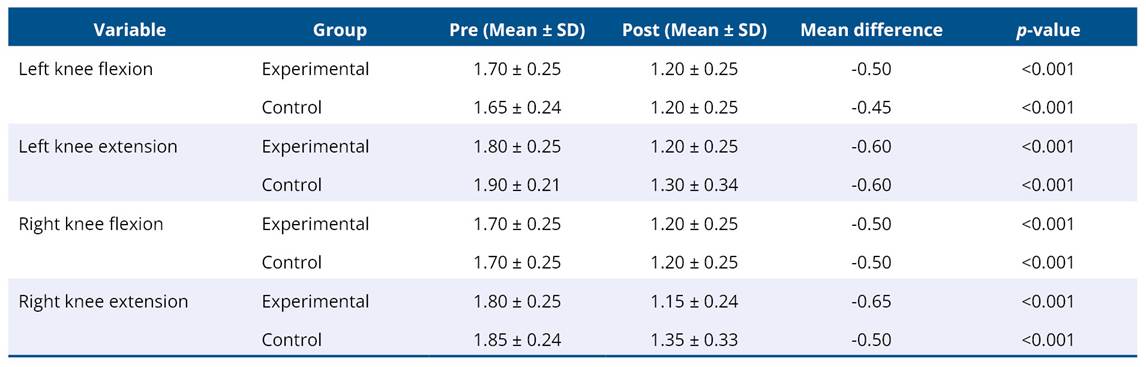
Table 5. Between-group comparison of post-intervention MAS

Table 6. Within-group changes in knee range of motion (degrees)
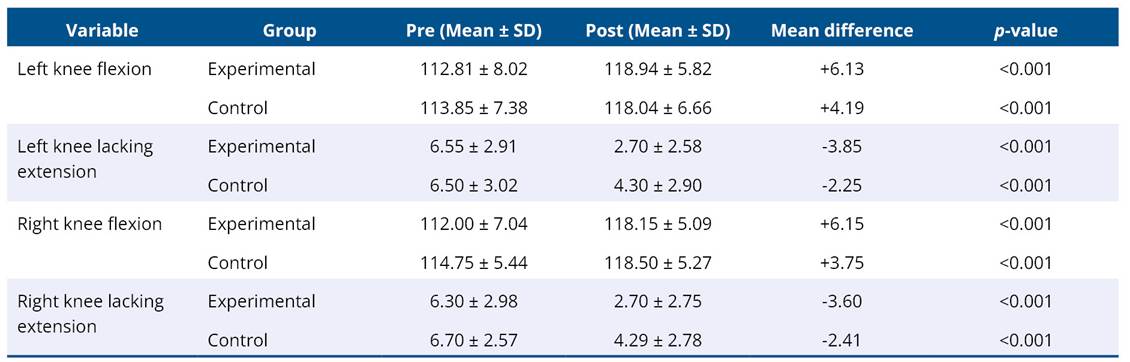
Table 7. Between-group comparison of post-intervention ROM

To prevent knee contractures and enhance knee extension range of motion (ROM) in children with diplegic spastic cerebral palsy, this randomized controlled trial (RCT) examined the effectiveness of kinesio taping and myofascial release interventions on hamstring spasticity. In this study, we focused on hamstring muscles due to their major involvement in knee flexion deformity, flexion contracture, and reduced knee extension. The results suggest significant within-group improvements in spasticity and knee range of motion were observed in both groups; however, no statistically significant between-group differences were found two weeks after the intervention.
A key finding was the comparatively larger effect sizes for knee extension and knee lacking extension variables than for knee flexion parameters. Moderate effect sizes were observed for right knee extension on MAS (d = 0.69) and for ROM lacking extension (d = 0.57–0.58), whereas flexion outcomes demonstrated negligible-to-small effects (d = 0–0.14). Post hoc power was also higher for extension-related variables (0.88–0.96), indicating greater sensitivity to detect moderate effects.
This pattern is clinically plausible. In spastic diplegic cerebral palsy, hamstring spasticity primarily restricts terminal knee extension rather than flexion range4,24. Because both MFR and KT were applied directly to the hamstrings, their inhibitory and mechanical effects are more likely to reduce resistance during passive extension, when the muscle is maximally stretched7. The Modified Ashworth Scale assesses resistance to passive movement; thus, reductions in hypertonicity would be more apparent during extension than flexion.
MFR may decrease fascial stiffness and improve tissue extensibility, particularly at end range, while KT applied from insertion to origin may provide inhibitory sensory input and modulate neuromuscular activation8,18,25. These mechanisms may explain the observed improvements in extension-related outcomes; however, since no significant between-group differences were found, these effects cannot be attributed specifically to the combined intervention. In contrast, knee flexion range is often relatively preserved in this population, potentially creating a ceiling effect that limits measurable improvement24.
This study shows similarity with the findings of Rasool et al. who reported that spasticity among CP children could be reduced by cross-friction massage when added to conventional physiotherapy26. Likewise, Tikhile et al. demonstrated that the combined effect of cryotherapy and myofascial stretching helped in reducing spasticity in calf muscles and improved ankle ROM10. Our findings are consistent with previous studies reporting improvements following myofascial release and other adjunct therapies; however, in the present study, these improvements were observed within groups, and no additional benefit over conventional therapy alone was demonstrated12,18,20.
A study done by Kaya Kara et al. demonstrated that the kinesio taping technique could enhance proprioceptive feedback and gross motor function in children with unilateral spastic cerebral palsy27. Previous studies have reported improvements in GMFM, gait parameters, and other outcomes with Kinesio taping; however, the present study did not demonstrate superior effects compared to conventional therapy alone14,15,28–32.
Tabatabaee et al. found no improvements in balance following a two-day taping intervention; however, they reported positive effects after a two-week intervention33. Although previous meta-analyses have reported positive effects of Kinesio taping on functional capacity, the present study did not demonstrate statistically significant superiority of the combined intervention over conventional therapy17.
Post hoc power analysis revealed that most MAS variables had low achieved power (≤0.50), suggesting that the study was underpowered to detect small between group effects. Although moderate effect sizes were observed for certain ROM variables, only right knee lacking extension demonstrated adequate power (>0.80).
The absence of statistically significant between-group differences may be influenced by the small sample size; however, based on the current findings, superiority of the combined intervention over conventional therapy cannot be concluded. The findings are limited to children with spastic diplegic cerebral palsy within the specified age range included in this study. Extrapolation to other cerebral palsy subtypes, age groups, or functional levels should be undertaken cautiously, and broader studies are needed to enhance external validity. Future large scale randomized controlled trials with adequate power are required to confirm these findings.
These results suggest that both groups demonstrated improvements over time; however, the addition of myofascial release and Kinesio taping did not result in superior outcomes compared to conventional physiotherapy alone.
This study has limitations. Due to the small sample size, short intervention duration (two weeks) and no long-term follow-up limiting the generalizability of the findings. Assessment was restricted to the hamstrings muscle group in children with cerebral palsy, while other spastic muscle groups were not evaluated. Spasticity was measured using the Modified Ashworth Scale, which does not differentiate between neural and biomechanical components. Functional outcome measures such as the Gross Motor Function Measure were not included, and Gross Motor Function Classification System levels were not reported. Due to the nature of the intervention, therapists and participants could not be blinded, and assessor blinding may also have been compromised. An intention-to-treat analysis was not performed, which may limit the robustness of the findings. Future definitive trials should incorporate intention-to-treat principles to minimize attrition bias and strengthen methodological rigor.
5. Conclusion
This pilot randomized controlled trial demonstrated that both conventional therapy alone and conventional therapy combined with kinesio taping and myofascial release resulted in significant within-group improvements in hamstring spasticity and knee range of motion. However, no statistically significant between-group differences were observed.
These findings indicate that improvements occurred in both groups; however, the combined intervention did not demonstrate superior short-term benefits compared to conventional therapy alone. Larger, adequately powered trials with longer follow-up periods are required to confirm these preliminary findings. Therefore, the findings of this study should be interpreted as evidence of within-group improvement rather than superiority of the combined intervention.
Data availability statement
Data will be made available upon request through the corresponding author. Dataset available at the Mendeley depository.doi: 10.17632/zg2xhgpt9d.1.
AI use disclosure
AI-assisted tools were used only for language editing and grammar correction. The authors performed all other activities.
Funding
There is no funding.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Bax MC. Terminology and classification of cerebral palsy. Dev Med Child Neurol. 1964;6(3):295–7. https://doi.org/10.1111/j.1469-8749.1964.tb10791.x
2. Patel DR, Bovid KM, Rausch R, Ergun-Longmire B, Goetting M, Merrick J. Cerebral palsy in children: a clinical practice review. Curr Probl Pediatr Adolesc Health Care. 2024;54(11):101673. https://doi.org/10.1016/j.cppeds.2024.101673
3. Chauhan A, Singh M, Jaiswal N, Agarwal A, Sahu JK, Singh M. Prevalence of cerebral palsy in Indian children: a systematic review and meta-analysis. Indian J Pediatr. 2019;86(12):1124–30. https://doi.org/10.1007/s12098-019-03024-0
4. Tang-Wai R, Webster RI, Shevell MI. A clinical and etiologic profile of spastic diplegia. Pediatr Neurol. 2006;34(3):212–8. https://doi.org/10.1016/j.pediatrneurol.2005.08.027
5. Tilton A. Management of spasticity in children with cerebral palsy. Semin Pediatr Neurol. 2004;16(2):82-9. https://doi.org/10.1016/j.spen.2009.03.006
6. Gorter JW, Rosenbaum PL, Hanna SE, Palisano RJ, Bartlett DJ, Russell DJ, et al. Limb distribution, motor impairment, and functional classification of cerebral palsy. Dev Med Child Neurol. 2004;46(7):461–7. https://doi.org/10.1111/j.1469-8749.2004.tb00506.x
7. Lieber RL, Steinman S, Barash IA, Chambers H. Structural and functional changes in spastic skeletal muscle. Muscle Nerve. 2004;29(5):615–27. https://doi.org/10.1002/mus.20059
8. Tabatabaee M, Cheraghifard M, Shamsoddini A. The effects of kinesio taping of lower limbs on functional mobility, spasticity, and range of motion of children with spastic cerebral palsy. Egypt J Neurol Psychiatr Neurosurg. 2019;55:70. https://doi.org/10.1186/s41983-019-0118-3
9. Morris D, Jones D, Ryan H, Ryan CG. The clinical effects of Kinesio® Tex taping: A systematic review. Physiother Theory Pract. 2013;29(4):259-70. https://doi.org/10.3109/09593985.2012.731675
10. Tikhile PJ, Bele AW. A protocol on effect of cryotherapy and myofascial release technique in calf muscle spasticity of spastic diplegic cerebral palsy children. Indian J Forensic Med Toxicol. 2021;15(2):587-91. https://doi.org/10.37506/ijfmt.v15i2.14374
11. Ryan JM, Cassidy EE, Noorduyn SG, O’Connell NE. Exercise interventions for cerebral palsy. Cochrane Database Syst Rev. 2017;6:CD011660. https://doi.org/10.1002/14651858.cd011660.pub2
12. Novak I, McIntyre S, Morgan C, Campbell L, Dark L, Morton N, et al. A systematic review of interventions for children with cerebral palsy: state of the evidence. Dev Med Child Neurol. 2013;55(10):885–910. https://doi.org/10.1111/dmcn.12246
13. Wu M, Kim J, Gaebler-Spira D. Improving trunk posture control in children with CP through a cable-driven robotic hippotherapy: A randomized controlled feasibility study. Gait Posture. 2024;113:209–14. https://doi.org/10.1016/j.gaitpost.2024.06.020
14. Şimşek TT, Türkücüoğlu B, Çokal N,Üstünbaş G, Şimşek IE. The effects of Kinesio® taping on sitting posture, functional independence and gross motor function in children with cerebral palsy. Disabil Rehabil. 2011;33(21–22):2058–63. https://doi.org/10.3109/09638288.2011.560331
15. Banerjee SB. Effect of kinesio taping on posture, balance and gait in spastic cerebral palsy - A systematic review. Med J DY Patil Vidyapeeth. 2024;17(3):507–14. https://doi.org/10.4103/mjdrdypu.mjdrdypu_483_23
16. Abbas ZU, Ahmed U, Sharif F, Siddique K, Shan e Fatima S, Ajmal M. Effects of routine physical therapy with and without kinesio taping in improving gross motor function in sitting and standing in spastic diplegic cerebral palsy children. J Bodyw Mov Ther. 2024;39:666–72. https://doi.org/10.1016/j.jbmt.2023.11.049
17. Lin X, Zhang J, Wu M, Li J, Song W, Zhu L. The effect of kinesio taping on motor function in children with cerebral palsy: a systematic review and meta-analysis of randomized controlled trials. Front Neurol. 2025;16:1527308. https://doi.org/10.3389/fneur.2025.1527308
18. Ajimsha MS, Al-Mudahka NR, Al-Madzhar JA. Effectiveness of myofascial release: Systematic review of randomized controlled trials. J Bodyw Mov Ther. 2015;19(1):102–12. https://doi.org/10.1016/j.jbmt.2014.06.001
19. Bhalara A, Talsaniya D. Short term effect of myofascial release on Calf muscle spasticity in spastic cerebral palsy patients. Int J Health Sci Res [Internet]. 2014;4(9):188. Available from: https://www.ijhsr.org/IJHSR_Vol.4_Issue.9_Sep2014/30.pdf
20. Paul J, Nathan SCV, Kumar P, Remya KR. Effectiveness of myofascial release in reduction of hamstrings spasticity among diplegic cerebral palsy children. Int J Med Exerc Sci [Internet]. 2018;4(1):453–8. Available from: https://ijmaes.org/wp-content/uploads/2019/10/2.Full-Text.pdf
21. Abdulazeez MU, Alhefeiti M, Alhammadi S, Alnuaimi H, Abdullahi AS, Shaikhoun L, et al. Normative knee range of motion for children. Life. 2025;15(7):1000. https://doi.org/10.3390/life15071000
22. Mutlu A, Livanelioglu A, Gunel MK. Reliability of Ashworth and Modified Ashworth Scales in children with spastic cerebral palsy. BMC Musculoskelet Disord. 2008;9(1):44. https://doi.org/10.1186/1471-2474-9-44
23. Meseguer-Henarejos AB, Sanchez-Meca J, López-Pina JA, Carles-Hernandez R. Inter-and intra-rater reliability of the Modified Ashworth Scale: A systematic review and meta-analysis. Eur J Phys Rehabil Med. 2018;54(4):576-90. https://doi.org/10.23736/s1973-9087.17.04796-7
24. Bartonek Å, Lidbeck C. Knee flexion while walking exceeds knee flexion contracture in children with spastic cerebral palsy. Children. 2023;10(12):1867. https://doi.org/10.3390/children10121867
25. Cunha AB, Lima-Alvarez CD, Rocha AC, Tudella E. Effects of elastic therapeutic taping on motor function in children with motor impairments: a systematic review. Disabil Rehabil. 2018;40(14):1609–17. https://doi.org/10.1080/09638288.2017.1304581
26. Rasool F, Memon AR, Kiyani MM, Sajjad AG. The effect of deep cross friction massage on spasticity of children with cerebral palsy: A double-blind randomised controlled trial. J Pak Med Assoc. 2017;67(1):87–91. Cited: PMID: 28065961
27. Kaya Kara O, Atasavun Uysal S, Turker D, Karayazgan S, Gunel MK, Baltaci G. The effects of kinesio taping on body functions and activity in unilateral spastic cerebral palsy: A single-blind randomized controlled trial. Dev Med Child Neurol. 2015;57(1):81–8. https://doi.org/10.1111/dmcn.12583
28. Çelik TÖ, Borman P, Tayman C, Kavakçi M, Çelebi F, Yaşar E. Effects of kinesiology taping on swallowing functions in newborns with swallowing difficulties: a randomized controlled pilot study. Rev Assoc Med Bras. 2023;69(10):e20230383. https://doi.org/10.1590/1806-9282.20230383
29. Mokhlesin M, Mirmohammadkhani M, Tohidast SA. The effect of kinesio taping on drooling in children with intellectual disability: A double-blind randomized controlled study. Int J Pediatr Otorhinolaryngol. 2022;153:111017. https://doi.org/10.1016/j.ijporl.2021.111017
30. Rastil ZA, Shamsoddini A, Dalvand H, Labaf S. The effect of kinesio taping on handgrip and active range of motion of hand in children with cerebral palsy. Iran J Child Neurol. 2017;11(4):43. Cited: PMID: 29201123
31. Balci NC, Ince DA, Ecevit A, Erdoğan B, Doğan IE, Turan O, et al. Impact of kinesio taping on oral feeding and swallowing functions: acoustic analysis of swallowing sounds in late preterm infants-a randomized clinical trial. Children. 2025;12(3):369. https://doi.org/10.3390/children12030369
32. Footer CB. The effects of therapeutic taping on gross motor function in children with cerebral palsy. Pediatr Phys Ther. 2006;18(4):245–52. https://doi.org/10.1097/01.pep.0000233696.33675.37
33. Tabatabaee M, Shamsoddini A, Cheraghifard M. Effects of lower limbs Kinesio taping on balance ability in children with cerebral palsy: A pilot randomized clinical trial. Iran Rehabil J. 2019;17(2):157–64.
