Original article
The silent strain: a cross-sectional study on postural biomechanical alterations and musculoskeletal health in security guards / A tensão silenciosa: um estudo transversal sobre alterações biomecânicas posturais e saúde musculoesquelética em vigilantes
Nidhi Sharma1 (https://orcid.org/0000-0003-3999-1780)
Anamika Kundu2 (https://orcid.org/0009-0008-3232-2545)
Simranjeet Kaur3 (https://orcid.org/0000-0002-0130-6437)
1Amity Institute of Health and Allied Sciences (Noida). Uttar Pradesh, India.
2Therafit Clinic (Siliguri). West Bengal, India.
3Corresponding contact. Pal Healthcare (Ambala). Haryana, India. [email protected]
ABSTRACT | BACKGROUND: Security guards often remain in prolonged static standing positions, predisposing them to subtle postural deviations and musculoskeletal pain. Despite this occupational risk, few studies have comprehensively examined these associations. OBJECTIVE: To investigate postural deviations in the anterior, posterior, and sagittal planes using photogrammetry and to explore their correlation with musculoskeletal pain among male security guards. METHODS: A cross-sectional study was conducted over 12 months involving 100 male security guards aged 30–50 years. Postural variables were analyzed using the Advanced Postural and Environmental Correction System (APECS) software through digital photogrammetry, while pain and symptoms were evaluated using the Nordic Musculoskeletal Questionnaire (NMQ) and the Numeric Pain Rating Scale (NPRS). Statistical analysis included descriptive statistics and Spearman’s rank correlation with Benjamini–Hochberg correction. RESULTS: Significant postural deviations were observed, particularly in shoulder and body alignment across the anterior and posterior coronal planes (r = 0.612, p < 0.001; r = 0.524, p < 0.001). A moderate correlation was found between ASIS inclination and lower back pain (r = 0.442, p = 0.002), while PSIS inclination showed a weak association (r = 0.260, p = 0.072). Other postural variables demonstrated weak or non-significant correlations with musculoskeletal pain. CONCLUSION: Despite evident postural asymmetries, only weak to moderate associations with musculoskeletal pain were identified. These findings highlight the multifactorial nature of occupational pain and underscore the need for ergonomic modifications and movement variability in preventive programs.
KEYWORDS: Cross-Sectional Studies. Musculoskeletal Pain. Ergonomics. Occupational Health. Posture.
RESUMO | INTRODUÇÃO: Os seguranças frequentemente permanecem em posições estáticas prolongadas em pé, o que os predispõe a desvios posturais sutis e dores musculoesqueléticas. Apesar desse risco ocupacional, poucas pesquisas examinaram essas associações de forma abrangente. OBJETIVO: Investigar os desvios posturais nos planos anterior, posterior e sagital usando fotogrametria e explorar sua correlação com a dor musculoesquelética entre seguranças do sexo masculino. MÉTODOS: Um estudo transversal foi conduzido ao longo de 12 meses, envolvendo 100 seguranças masculinos com idades entre 30 e 50 anos. As variáveis posturais foram avaliadas utilizando o software Advanced Postural and Environmental Correction System (APECS) através de fotogrametria digital, enquanto a dor e os sintomas foram avaliados utilizando o Nordic Musculoskeletal Questionnaire (NMQ) e a Numeric Pain Rating Scale (NPRS). A análise estatística incluiu estatísticas descritivas e correlação de postos de Spearman com correção de Benjamini–Hochberg. RESULTADOS: Foram encontrados desvios posturais significativos, especialmente no alinhamento dos ombros e do corpo nos planos coronais anterior e posterior (r = 0,612, p < 0,001; r = 0,524, p < 0,001). Uma correlação moderada foi observada entre a inclinação da EIAS (espinha ilíaca anterossuperior) e a dor lombar (r = 0,442, p = 0,002), enquanto a inclinação da EIPS (espinha ilíaca posterossuperior) mostrou uma correlação fraca (r = 0,260, p = 0,072). Outras variáveis posturais apresentaram correlações fracas ou não significativas com a dor musculoesquelética. CONCLUSÃO: Apesar das assimetrias posturais evidentes, apenas associações fracas a moderadas com a dor musculoesquelética foram observadas. Os achados reforçam a natureza multifatorial da dor ocupacional e destacam a importância de modificações ergonômicas e da variabilidade de movimento na prevenção da dor.
PALAVRAS-CHAVE: Estudos Transversais. Dor Musculoesquelética. Ergonomia. Saúde Ocupacional. Postura.
How to cite this article: Sharma N, Kundu A, Kaur S. The silent strain: a cross-sectional study on postural biomechanical alterations and musculoskeletal health in security guards. J Physiother Res. 2026;16:e6498. https://doi.org/10.17267/2238-2704rpf.2026.e6498
Submitted 7 Oct., 2025, Accepted 9 Dec., 2025, Published 23 Mar., 2025
J. Physiother. Res., Salvador, 2026;16:e6498
https://doi.org/10.17267/2238-2704rpf.2026.e6498
ISSN: 2238-2704
Assigned editor: Marina Portugal Makhoul
1. Introduction
Musculoskeletal disorders (MSDs) are a leading cause of disability and absenteeism globally, particularly in jobs requiring prolonged standing or fixed body postures3. Poor alignment, such as excessive anterior pelvic tilt or scapular asymmetry, may contribute to localized discomfort or overuse injuries4. However, emerging evidence suggests that posture alone does not determine pain; it is one of several interacting factors5-7.
Modern perspectives emphasize that musculoskeletal pain is multifactorial—resulting from not just biomechanical stress but also ergonomic, psychosocial, and behavioral influences8-10. In the context of security personnel, prolonged static standing can exacerbate spinal compression, reduce muscular pump action, and increase loading of the posterior kinetic chain, especially in the lumbar spine11,12.
Photogrammetry has gained attention as a valid and non-invasive tool for analyzing posture in clinical and field settings13,14. It enables angle-based quantification of postural deviations across multiple anatomical planes. However, few studies have examined whether such deviations are meaningfully linked to musculoskeletal pain, particularly among security guards in the Indian context, where ergonomic awareness and workplace training may be limited.
This study aimed to investigate the association between static postural deviations and musculoskeletal pain among male security guards with occupational exposure to prolonged standing (defined as standing for more than four hours daily for at least three years).
2. Method
2.1 Ethical considerations
Ethical clearance was granted by the Institutional Ethics Committee (Approval No. IEC/MMDU/2421) on 30/04/2023. The study was registered with the Clinical Trials Registry (Trial No. CTRI/2023/07/054965). Ethical standards consistent with the Declaration of Helsinki and Indian Council of Medical Research guidelines were followed.
2.2 Study design and participants
This cross-sectional study was conducted over 12 months (March 2023 – February 2024) at a private university. A total of 100 male security guards aged 30–50 years were recruited using convenience sampling. Participants were included only if they routinely stood for more than four hours per workday and had at least three years of continuous experience in security duties, ensuring adequate exposure to prolonged static standing. Only male security guards were included in the study, as all security personnel employed at the study site during the data collection period were male. This was a practical decision based on the available population rather than a predefined exclusion criterion. Exclusion criteria encompassed spinal injuries, orthopedic or neurological disorders, and congenital deformities.
2.3 Sample size
Sample size was estimated using a single proportion formula (n = (Zα)2p(1 – p)/d2) with 95% confidence, 10% margin of error, and 68% assumed prevalence1 accounting for 20% potential dropouts, the final sample size was 100.
2.4 Data collection tools and procedures
After obtaining informed consent, participants underwent a postural assessment using the Advanced Postural and Environmental Correction System (APECS Pro-PLUS v8.4.12), a validated photogrammetry software. Participants were photographed in standardized standing posture from anterior, posterior, and sagittal views with anatomical markers applied at key bony landmarks.
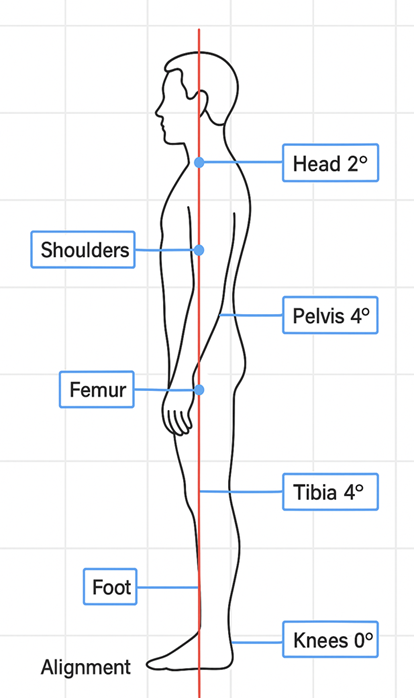
The following anatomical points and angles were analyzed:
· Anterior view: Head alignment (vertical), shoulder alignment (acromion level difference), ASIS (anterior superior iliac spine) inclination.
· Posterior view: PSIS (posterior superior iliac spine) inclination, body vertical alignment, scapular asymmetry.
· Sagittal view: Forward head angle, trunk inclination, pelvic tilt, and knee joint alignment.
· Foot rotation was observed for both limbs in the transverse plane.
A sample screenshot of the schematic line diagram interface (Figure 1a, 1b and 1c) is included to illustrate the measurement approach. Although we collected qualitative data on time spent in static standing posture via structured interviews, the responses lacked consistency and could not be statistically analyzed. This is acknowledged as a limitation.
Figure 1a: Screenshot from schematic line diagram showing anatomical points and angular measurements used in the photogrammetric posture analysis (Anterior View)
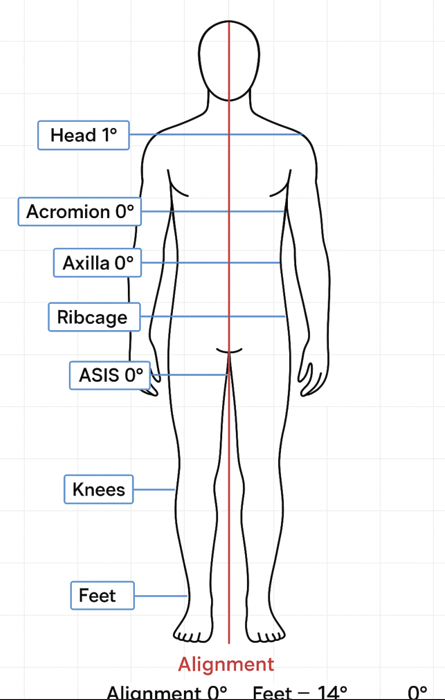
Figure 1b: Screenshot from schematic line diagram showing anatomical points and angular measurements used in the photogrammetric posture analysis (Posterior View)
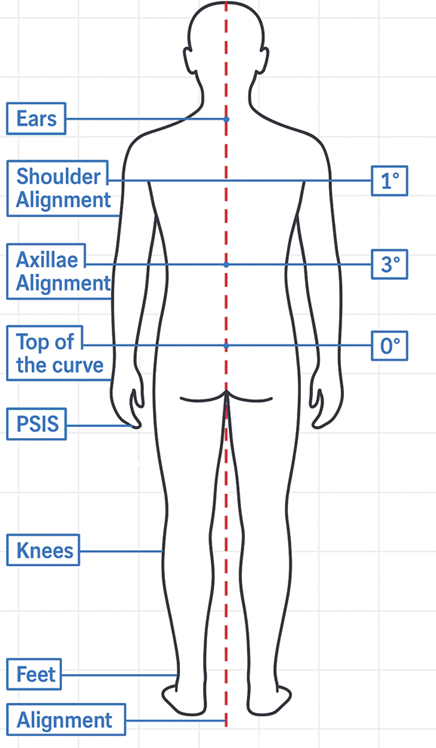
Figure 1c: Screenshot from schematic line diagram showing anatomical points and angular measurements used in the photogrammetric posture analysis (Lateral View)
2.5 Instruments
The assessments were conducted by two assessors, one holding a Master’s degree in Physiotherapy with six years of clinical and research experience in musculoskeletal evaluation and one is a postgraduate student of Master’s degree in Physiotherapy. Both assessors were trained in the standardized administration of the APECS software (Pro-PLUS v8.4.12), Nordic Musculoskeletal Questionnaire (NMQ) and the Numeric Pain Rating Scale (NPRS) prior to the commencement of data collection to ensure consistency and inter-rater reliability.
The assessments took place in a quiet, well-ventilated occupational health room located within the premises of the respective security offices to maintain a familiar and comfortable environment for the participants. The space was free from distractions and equipped with adequate seating and lighting to facilitate the interview and form-filling process.
· Posture assessment: The Advanced Postural and Environmental Correction System (APECS Pro-PLUS v8.4.12) was used for photogrammetric analysis of static posture. The software has demonstrated validated reliability for measuring angular deviations such as shoulder alignment, pelvic tilt, and trunk inclination in both clinical and occupational settings, with documented intra- and inter-rater reliability (ICC > 0.85) for hip–knee–ankle and trunk inclination measures15-17.
Recent studies using digital and AI-based posture assessment platforms have confirmed similar reliability and reproducibility, supporting the accuracy of non-radiographic postural evaluation methods16,18. The APECS software (Pro-PLUS v8.4.12) was used to assess postural alignment using anatomical landmarks across anterior coronal, posterior coronal, and sagittal planes15-17. While global posture analysis is widely adopted, reliability varies depending on marker placement and calibration; therefore, the present study focused on reproducible measures within those validated parameters.
· Musculoskeletal symptoms: The Nordic Musculoskeletal Questionnaire (NMQ) was used to determine the prevalence of pain in nine anatomical regions. The NMQ was administered in either self-report or interview format, depending on participant preference and literacy level, to record the presence and distribution of musculoskeletal symptoms over the past 12 months and the past 7 days. The original NMQ demonstrated good test–retest reliability (κ = 0.70–0.89) and strong content validity, established through expert consensus across multiple Nordic countries which is reliable for both clinical and research settings19.
· Pain intensity: NPRS assessed self-reported pain on a scale from 0 (no pain) to 10 (worst imaginable pain)20. It is a standardized tool developed to identify the prevalence and distribution of musculoskeletal symptoms in various body regions over specific time frames. Participants are asked “Please rate your pain by choosing a number from 0 to 10 that best represents your pain intensity right now"8.
The entire data collection for each participant took approximately 15–20 minutes. Completed forms were reviewed immediately by the assessors to ensure completeness and clarify any inconsistencies. The validity has demonstrated excellent test–retest reliability (ICC = 0.95–0.98) and strong construct validity through high correlations with other established pain scales (r = 0.86–0.95)21.
2.6 Statistical analysis
Data were analyzed using IBM SPSS Statistics, version 20. Descriptive statistics (mean, standard deviation, and 95% confidence intervals) were calculated for all postural and pain variables.
The relationships between postural parameters and musculoskeletal pain were examined using Spearman’s rank correlation coefficient, as data were not normally distributed. To control for potential inflation of Type I error due to multiple correlation testing, the Benjamini–Hochberg false discovery rate (FDR) correction was applied, with the FDR set at 5%.
All statistical tests were two-tailed, and a p value ≤ 0.05 was considered statistically significant.
3. Results
A total of 100 male security guards participated in the study. The mean age was 42.6 ± 5.9 years, with a mean body mass index (BMI) of 23.2 ± 2.1 kg/m². Most demographic variables were normally distributed (p > 0.05), except years of experience and standing duration (p < 0.05). Participants reported standing for an average of 6.2 ± 1.9 hours per day and had an average of 8.5 ± 3.7 years of professional experience. Approximately one-third engaged in regular physical activity (34%), while 12% reported being current smokers. Nine participants (9%) indicated known medical comorbidities such as hypertension or diabetes (Table 1).
Table 1. Demographic and occupational characteristics of participants (n = 100)
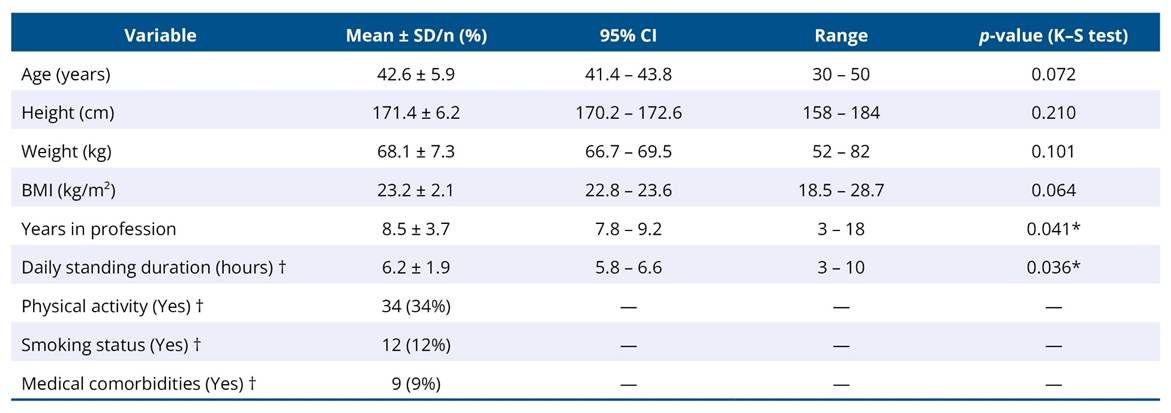
*p < 0.05 indicates deviation from normal distribution (Kolmogorov–Smirnov test). †Self-reported estimates.
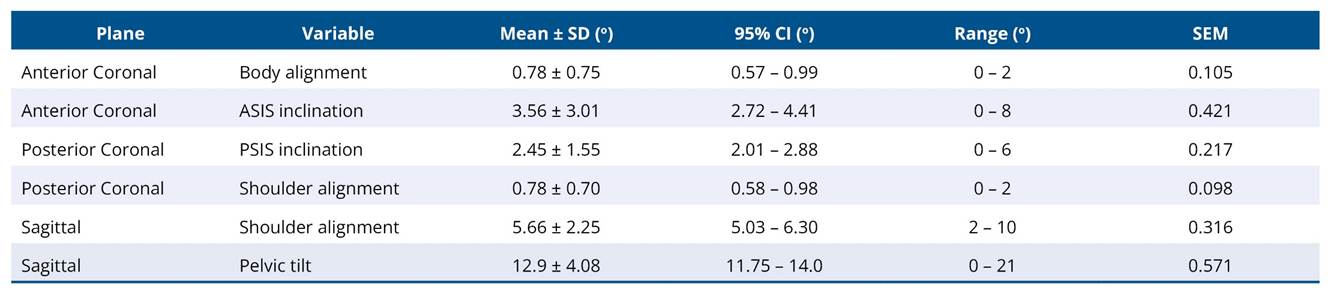
3.1 Postural deviations
Photogrammetric analysis using the APECS Pro-PLUS v8.4.12 software revealed measurable deviations across several key postural variables (Table 2). The mean anterior superior iliac spine (ASIS) inclination was 3.56° ± 3.01°, posterior superior iliac spine (PSIS) inclination was 2.45° ± 1.55°, and pelvic tilt in the sagittal plane was 12.9° ± 4.08°. Shoulder alignment deviation averaged 5.66° ± 2.25° in the sagittal plane.
These findings indicate mild-to-moderate postural asymmetries consistent with
anterior pelvic rotation and upper body compensations frequently reported in
occupations involving prolonged standing.
Table 2. Descriptive statistics of postural variables (n = 100)
3.2 Inter-planar correlations
Correlations among postural variables across anatomical planes are presented in Table 3. Shoulder alignment in the anterior and posterior coronal planes demonstrated a strong positive correlation (r = 0.612, p < 0.001, FDR-adjusted). Body alignment across the same planes showed a moderate correlation (r = 0.524, p < 0.001). Significant associations were also observed between ASIS and PSIS inclinations (r = 0.337, p = 0.019). These results suggest coordinated deviations between anterior and posterior body segments, consistent with a systemic postural adaptation pattern
Table 3. Correlation of postural variables across anatomical planes (Benjamini–Hochberg Adjusted)
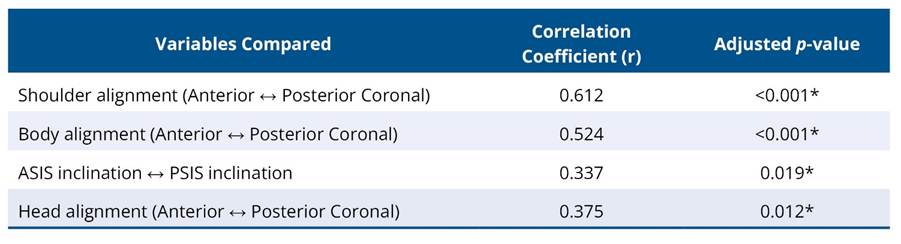
*Significant at FDR-adjusted p < 0.05.
3.3 Correlation between posture and musculoskeletal pain
Correlations between postural deviations and musculoskeletal pain, assessed using the Nordic Musculoskeletal Questionnaire (NMQ) and the Numeric Pain Rating Scale (NPRS), are shown in Table 4. The strongest association was between ASIS inclination and lower back pain (r = 0.442, p = 0.002, FDR-adjusted). PSIS inclination showed a weak, non-significant association (r = 0.260, p = 0.072). No significant correlations were observed for pelvic tilt or shoulder alignment with pain intensity. Right foot rotation was inversely correlated with ankle pain (r = −0.297, p = 0.041).
Table 4. Correlation between postural variables and musculoskeletal pain
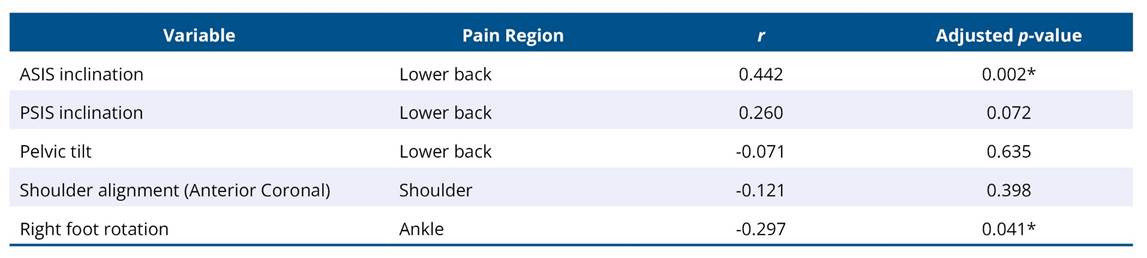
*Significant at FDR-adjusted p < 0.05.
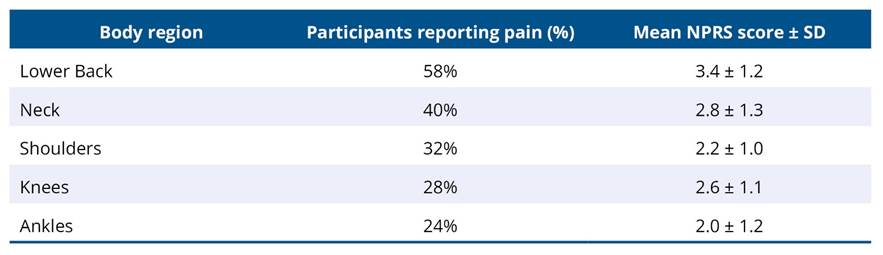
3.4 Pain prevalence and intensity
Pain distribution across anatomical regions is summarized in Table 5. The lower back was the most frequently affected region (58%), with a mean pain intensity of 3.4 ± 1.2 on the Numeric Pain Rating Scale (NPRS), followed by the neck (40%) and shoulders (32%). The mean pain intensity ranged from 2.0 – 3.4 across regions, indicating mild to moderate discomfort.
Table 5. Distribution of Pain by body region (NMQ) and Mean pain intensity (NPRS)
3.5 Static standing time
Although participants were asked to estimate the average number of hours spent in static standing each day, the responses were inconsistent and lacked precision. Consequently, this variable was not included in the statistical analysis. Future studies should employ objective monitoring tools (e.g., wearable devices or activity logs) to quantify exposure duration more reliably.
3.6 Summary of key findings
Table 6 presents an overview of significant correlations and observed patterns for ease of interpretation.
Table 6. Summary of significant postural deviations and correlations

The analyses presented were descriptive and correlational in nature, and no causal inferences were drawn from the data. As the sample consisted exclusively of male participants from a single institution, the findings should be interpreted with caution and may not generalize to broader populations. Additionally, potential confounding factors such as BMI, physical activity level, and years of professional experience were not controlled for, which is recognized as a limitation and further discussed below.
4. Discussion
This cross-sectional study examined the relationship between static postural deviations and musculoskeletal pain among male security guards routinely exposed to prolonged standing. The analysis revealed measurable postural asymmetries—particularly in anterior superior iliac spine (ASIS) inclination, posterior superior iliac spine (PSIS) inclination, pelvic tilt, and shoulder alignment. Despite these deviations, only weak to moderate correlations were observed between postural parameters and reported pain, supporting the multifactorial nature of musculoskeletal discomfort.
Among the evaluated variables, the most notable relationship was between ASIS inclination and lower back pain. This association is biomechanically plausible, as anterior pelvic tilt can increase lumbar lordosis and spinal loading, thereby heightening mechanical stress on posterior structures22. However, other deviations, such as PSIS inclination and shoulder alignment, showed no meaningful association with pain severity, reflecting the current understanding that posture alone does not fully explain musculoskeletal symptoms12,13.
Significant correlations observed between anterior and posterior shoulder alignment suggest systemic adaptation across body segments rather than isolated distortions. This pattern of compensatory alignment may help maintain balance during prolonged static standing but does not necessarily predict pain intensity4,5. Prior research indicates that factors such as ergonomics, psychological stress, and activity variability often play a larger role than static posture itself in the development of musculoskeletal symptoms3,7.
The most frequent pain site among participants was the lower back (58%), followed by the neck and shoulders. However, pain intensity levels were generally mild to moderate, suggesting a chronic, low-grade strain rather than acute pathology. This finding supports the concept of “silent strain”—a gradual, subclinical accumulation of tissue stress during prolonged standing2,11. Over time, such strain can predispose workers to discomfort and functional limitations even in the absence of overt injury.
Although this study was cross-sectional, data were collected over twelve months (March 2023–February 2024) due to logistical constraints. This extended collection window could have introduced minor variability related to seasonal or occupational changes10. Future cross-sectional research should consider shorter data collection periods (e.g., 2–3 months) to minimize such confounding factors.
The inclusion criteria ensured participants had long-term exposure to static standing (more than four hours daily for over three years). However, standing duration was self-reported and not objectively measured. Variability in these estimates limited their reliability, and thus the variable was excluded from analysis. Future research should employ wearable motion sensors or activity logs to record standing duration and posture dynamics more accurately26.
All participants were male employees from a single institution, which restricts the generalizability of findings to broader or gender-diverse populations15. Additionally, factors such as age, body mass index (BMI), years of professional experience, and physical activity levels were not statistically controlled for in the analyses. These potential confounders may influence both postural alignment and pain perception23,24.
Taken together, these findings suggest that while measurable postural deviations exist among individuals in prolonged standing occupations, they alone do not predict pain intensity or distribution. This aligns with contemporary models of occupational pain emphasizing that musculoskeletal symptoms emerge from a combination of biomechanical, ergonomic, and psychosocial factors1,6,14.
To effectively manage and prevent discomfort in security personnel and similar occupations, interventions should extend beyond simple postural correction. A more comprehensive strategy could include ergonomic redesign of standing workstations14, scheduled dynamic movement or micro-breaks25, and educational initiatives to improve postural awareness and body mechanics27.
Limitations and future directions
This study has certain limitations that should be acknowledged. The sample consisted exclusively of male security guards from a single institution, which restricts the generalizability of findings to other occupational or gender groups15. Although inclusion criteria ensured long-term exposure to static standing (>4 hours daily for over three years), the data were self-reported and not objectively measured, which may have introduced recall bias26. Additionally, potential confounding factors such as age, body mass index, physical activity level, and years of experience were not controlled for, limiting the strength of causal interpretation23,24.
The cross-sectional design captures associations but cannot determine cause-and-effect relationships13,22. Pain and symptoms were assessed through self-reported tools (NMQ and NPRS)8,9, which, despite being validated, remain subjective. Future studies should integrate objective biomechanical assessments such as electromyography, wearable posture sensors, or motion analysis to complement self-reported measures.
Further research should include gender-diverse and multi-institutional samples, employ dynamic posture tracking to quantify standing exposure, and analyze ergonomic and psychosocial influences comprehensively1,25. Preventive strategies including workstation redesign, periodic movement breaks, and postural education programs27 may enhance musculoskeletal resilience in occupations requiring prolonged standing.
5. Conclusion
In conclusion, although postural asymmetries were common among the security guards studied, their association with musculoskeletal pain was only weak to moderate. Certain patterns—such as increased anterior pelvic tilt—were linked with low back discomfort, but posture alone did not explain pain occurrence22. Future studies should include both male and female workers, quantify static standing duration objectively26, and employ longitudinal designs to better elucidate how posture and pain evolve over time.
Use of AI tools
During the preparation of this manuscript, the authors utilized ChatGPT (OpenAI, San Francisco, USA) to assist in enhancing the clarity and coherence of the text. All scientific content, interpretation, and conclusions were made by the authors. The final manuscript was reviewed and approved by all authors.
Acknowledgement
Authors would like to acknowledge Maharishi Markandeshwar – Deemed to be University (Mullana-Ambala), Haryana, India for providing the infrastructure required for the conduction of the trial.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Kaur S, Sudhakar K, Gupta S. To study the prevalence of musculoskeletal disorders in security guards. Int J Physiother. 2015;2(6):905-10. https://doi.org/10.15621/ijphy/2015/v2i6/80747
2. Nelson-Wong E, Callaghan JP. The impact of a sloped surface on low back pain during prolonged standing work: a biomechanical analysis. Ergonomics. 2010;53(8):953-61. https://doi.org/10.1016/j.apergo.2010.01.005
3. Comper ML, Macedo AR, Padula RS. Musculoskeletal symptoms, postural disorders and occupational risk factors: correlation analysis. Work. 2012;41 Suppl 1:2445-8. https://doi.org/10.3233/wor-2012-0478-2445
4. Salahzadeh Z, Maroufi N, Ahmadi A, Behtash H, Razmjoo A, Parnianpour M. Assessment of forward head posture in females: observational and photogrammetric study. J Back Musculoskelet Rehabil. 2014;27(2):131-9. https://doi.org/10.3233/bmr-130426
5. Marinho MFS, Lucena LC. Postural changes and chronic lumbar pain in university students: original study. Coluna/Columna. 2022;21(4):2-7. https://doi.org/10.1590/S1808-185120222104261566
6. Saad KR, Colombo AS, Ribeiro AP, João SM. Reliability of photogrammetry in the evaluation of the postural aspects of individuals with structural scoliosis. J Bodyw Mov Ther. 2012;16(2):210-6. https://doi.org/10.1016/j.jbmt.2011.03.005
7. Furlanetto TS, Sedrez JA, Candotti CT, Loss JF. Photogrammetry for the evaluation of spinal posture: a systematic review. J Bodyw Mov Ther. 2016;20(4):820-6. https://doi.org/10.5312/wjo.v7.i2.136
8. Dickinson CE, Campion K, Foster AF, Newman SJ, O'Rourke AMT, Thomas PG. Questionnaire development: an examination of the Nordic Musculoskeletal Questionnaire. Appl Ergon. 1992;23(3):197-201. https://doi.org/10.1016/0003-6870(92)90225-k
9. Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain. 2011;152(10):2399-404. https://doi.org/10.1016/j.pain.2011.07.005
10. Daly RM, Rosengren BE, Alwis G, Ahlborg HG, Sernbo I, Karlsson MK. Gender-specific age-related changes in bone density, muscle strength and functional performance in the elderly: a 10-year prospective population-based study. BMC Geriatr. 2013;13:71. https://doi.org/10.1186/1471-2318-13-71
11. Karimi Z, Mazloumi A, Sharifnezhad A, Jafari AH, Kazemi Z, Keihani A. Nonlinear analysis of postural changes related to movement interventions during prolonged standing tasks. Ergonomics. 2023;66(7):939-53. https://doi.org/10.1080/00140139.2023.2188732
12. Slater D, Korakakis V, O'Sullivan P, Nolan D, O'Sullivan K. "Sit Up Straight": Time to Re-evaluate. J Orthop Sports Phys Ther. 2019;49(8):562-4. https://doi.org/10.2519/jospt.2019.0610
13. O’Sullivan P. It’s time for change with the management of non-specific chronic low back pain. Br J Sports Med. 2012;46(4):224-7. https://doi.org/10.1136/bjsm.2010.081638
14. Mallapiang F, Azriful, Nildawati, Syarfaini, Muis M, Adriansyah. The relationship of posture working with musculoskeletal disorders (MSDs) in the weaver West Sulawesi Indonesia. Gac Sanit. 2021;35 Suppl 1:S15-8. https://doi.org/10.1016/j.gaceta.2020.12.005
15. Singla D, Veqar Z, Hussain ME. Photogrammetric Assessment of Upper Body Posture Using Postural Angles: A Literature Review. J Chiropr Med. 2017;16(2):131-8. https://doi.org/10.1016/j.jcm.2017.01.005
16. Çankaya M, Takı FN. Comparison of postural assessment and awareness in individuals receiving posture training using the digital AI posture assessment and correction system. Int J Occup Saf Ergon. 2024;30(4):1311-7. https://doi.org/10.1080/10803548.2024.2397836
17. Welling A, Gurudut P, Shirodkar G, Shetye N, Khan S. Validation of non-radiographic APECS software in comparison with standard radiographic measurement of full-length lower limb hip-knee-ankle angle in elderly obese women. Physiother Q. 2023;31(1):90-4. https://doi.org/10.5114/pq.2023.124567
18. Trovato B, Roggio F, Sortino M, Zanghì M, Petrigna L, Giuffrida R, et al. Postural evaluation in young healthy adults through a digital and reproducible method. J Funct Morphol Kinesiol. 2022;7(4):98. https://doi.org/10.3390/jfmk7040098
19. Kuorinka I, Jonsson B, Kilbom Å, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18(3):233-7. https://doi.org/10.1016/0003-6870(87)90010-X
20. Jensen MP, Karoly P. Self-report scales and procedures for assessing pain in adults. In: Turk DC, Melzack R, editors. Handbook of pain assessment. 2nd ed. New York: Guilford Press; 2001. p. 15-34.
21. Farrar JT, Young Jr JP, LaMoreaux L, Werth JL, Poole MR. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149-58. https://doi.org/10.1016/S0304-3959(01)00349-9
22. McGill SM. Low back disorders: evidence-based prevention and rehabilitation. 2nd ed. Champaign: Human Kinetics; 2007.
23. van Dieën JH, Reeves NP, Kawchuk G, van Dillen LR, Hodges PW. Motor control changes in low back pain: divergence in presentations and mechanisms. J Orthop Sports Phys Ther. 2019;49(6):370-9. https://doi.org/10.2519/jospt.2019.7917
24. O’Sullivan P. Diagnosis and classification of chronic low back pain disorders: maladaptive movement and motor control impairments as underlying mechanism. Man Ther. 2005;10(4):242-55. https://doi.org/10.1016/j.math.2005.07.001
25. Robertson MM, Ciriello VM, Garabet AM. Office ergonomics training and a sit-stand workstation: effects on musculoskeletal and visual symptoms and performance of office workers. Appl Ergon. 2013;44(1):73-85. https://doi.org/10.1016/j.apergo.2012.05.001
26. Coenen P, Willenberg L, Parry S, Shi JW, Romero L, Blackwood DM, et al. Associations of occupational standing with musculoskeletal symptoms: a systematic review with meta-analysis. Br J Sports Med. 2018;52(3):176-83. https://doi.org/10.1136/bjsports-2016-096795
27. Pehlevan E, Şevgin Ö. Effect of exercise given to factory workers with ergonomics training on pain and functionality: a randomized controlled trial. Work. 2024;78(1):195-205. https://doi.org/10.3233/wor-230663
