Case report
Functional evolution 18 months after selective dorsal rhizotomy in a child with bilateral cerebral palsy from Zona da Mata: case report / Evolução funcional 18 meses após rizotomia dorsal seletiva em uma criança com paralisia cerebral bilateral da Zona da Mata: relato de caso
Isabela de Pádua Ruiz1 (https://orcid.org/0009-0007-8553-3509)
Vanessa Aparecida Dias Chaves2 (https://orcid.org/0009-0007-2597-8709)
Leonardo Raphael Santos Rodrigues3 (https://orcid.org/0000-0002-6640-680X)
Júlia de Souza Castilho Silvério4 (https://orcid.org/0000-0002-9923-8857)
Rayla Amaral Lemos5 (https://orcid.org/0000-0003-3090-1806)
Paula Silva de Carvalho Chagas6 (https://orcid.org/0000-0002-4312-0403)
1,2,4,5Universidade Federal de Juiz de Fora (Juiz de Fora). Minas Gerais, Brazil.
3Universidade Estadual do Piauí (Teresina). Piauí, Brazil.
6Corresponding contact. Universidade Federal de Juiz de Fora (Juiz de Fora). Minas Gerais, Brazil. [email protected]
ABSTRACT | INTRODUCTION: Selective Dorsal Rhizotomy (SDR) is a neurosurgical intervention used to reduce spasticity in children with cerebral palsy (CP). Despite advances, SDR is still not widely disseminated, and the scarcity of reports limits the understanding of its functional impacts. OBJECTIVE: To describe the functional changes in a child with bilateral spastic CP, diplegic type, after SDR combined with physiotherapy. MATERIALS AND METHODS: Case report with longitudinal follow-up for 18 months of a 3-year-8-month-old male child, classified by the Gross Motor Function Classification System (GMFCS) as level III, who underwent SDR and intensive postoperative rehabilitation. Spasticity was assessed using the Modified Ashworth Scale, and functioning using the Gross Motor Function Measure (GMFM-66), preoperatively and every three months after surgery. GMFM-66 scores were analyzed using GMAE-3 software, which allowed for the estimation of Expected Natural Evolution (ENE) as a parameter to interpret gains over time. RESULTS: After surgery, a reduction in spasticity in the lower limbs was observed. In all postoperative assessments, variations in GMFM-66 scores were greater than the ENE, with a significant increase at three months (p<0.05), a period marked by the acquisition of motor skills previously limited by spasticity. CONCLUSION: SDR combined with physiotherapy and family involvement showed a reduction in spasticity and a significant increase in functioning and motor capacity. The child's active participation and parental involvement were key factors for the success of the treatment.
KEYWORDS: Rhizotomy. Cerebral Palsy. Functioning, Children with Disabilities. Motor Skills. Physical Therapy Modalities.
RESUMO | INTRODUÇÃO: A Rizotomia Dorsal Seletiva (RDS) é uma intervenção neurocirúrgica utilizada para a redução da espasticidade em crianças com paralisia cerebral (PC). Apesar dos avanços, a RDS ainda é pouco difundida, e a escassez de relatos limita a compreensão de seus impactos funcionais. OBJETIVO: Descrever as mudanças funcionais de uma criança PC bilateral espástica do tipo diplégica, após RDS associada à fisioterapia. MATERIAIS E MÉTODOS: Relato de caso com acompanhamento longitudinal por 18 meses de uma criança do sexo masculino, de 3 anos e 8 meses, classificada pelo Sistema de Classificação da Função Motora Grossa (GMFCS) como nível III, submetida à RDS e à reabilitação intensiva no pós-operatório. A espasticidade foi avaliada pela Escala de Ashworth Modificada, e a funcionalidade pela Medida da Função Motora Grossa (GMFM-66), no pré-operatório e a cada três meses após a cirurgia. Os escores do GMFM-66 foram analisados por meio do software GMAE-3, que permitiu a estimativa da Evolução Natural Esperada (ENE) como parâmetro para interpretar os ganhos ao longo do tempo. RESULTADOS: Após a cirurgia, observou-se redução da espasticidade nos membros inferiores. Em todas as avaliações pós-operatórias, as variações nos escores do GMFM-66 foram superiores à ENE, com aumento significativo aos três meses (p < 0,05), período marcado pela aquisição de habilidades motoras previamente limitadas pela espasticidade. CONCLUSÃO: A RDS, combinada com fisioterapia e envolvimento familiar evidenciou redução da espasticidade, aumento significativo da funcionalidade e da capacidade motora. A participação ativa da criança e o envolvimento dos pais foram fatores chave para o sucesso do tratamento.
PALAVRAS-CHAVE: Rizotomia. Paralisia Cerebral. Funcionalidade. Crianças com Deficiência. Habilidades Motoras. Fisioterapia.
How to cite this article: Ruiz IP, Chaves VAD, Rodrigues LRS, Silvério JSC, Lemos RA, Chagas PSC. Functional evolution 18 months after selective dorsal rhizotomy in a child with bilateral cerebral palsy from Zona da Mata: case report. J Physiother Res. 2026;16:e6494. https://doi.org/10.17267/2238-2704rpf.2026.e6494
Submitted Oct. 10, 2025, Accepted Mar. 6, 2026, Published Apr. 24, 2026
J. Physiother. Res., Salvador, 2026;16:e6494
https://doi.org/10.17267/2238-2704rpf.2026.e6494
ISSN: 2238-2704
Assigned editor: Juliana Goulardins
1. Introduction
Cerebral palsy (CP) is the leading cause of physical disability in childhood, with an estimated prevalence of 2 to 3 cases per 1,000 live births, representing an important public health issue1,2. It is a non-progressive condition, characterized by disorders of movement and posture, with heterogeneous clinical manifestations that may significantly impact functioning, participation, and quality of life of children and their families throughout life3. The diversity of clinical presentation imposes multifactorial challenges for both family care and the work of health professionals1.
Given the different motor manifestations of CP, spasticity is one of the most frequent and constitutes an important limiting factor for function4. Its management is complex and involves different therapeutic approaches, including pharmacological treatments, injectable procedures, and more invasive interventions, such as the intrathecal baclofen pump2. Although these strategies may provide benefits, many offer temporary solutions or are associated with relevant adverse effects, reinforcing the need for effective and sustainable therapeutic alternatives4.
In this context, Selective Dorsal Rhizotomy (SDR) stands out as an effective surgical alternative for the permanent reduction of spasticity5. It is an irreversible neurosurgical procedure that consists of the selective sectioning of the sensory dorsal roots of the spinal cord, aiming to interrupt pathological afferent impulses responsible for increased muscle tone2. Over the years, the technique has been refined and has become widely used in the management of spastic CP, especially in children with spastic diplegia classified in levels I to III of the Gross Motor Function Classification System (GMFCS), a group in which significant gains in gait and mobility have been reported5.
Scientific evidence indicates that the benefits of SDR go beyond the reduction of muscle tone, including improvements in motor performance, reduction of musculoskeletal deformities, pain relief, and facilitation of daily care provided by the family4,6. However, these benefits are associated with a structured and continuous rehabilitation process, in which physiotherapy plays a crucial role, particularly in the postoperative period7.
Despite the advances described in the literature, SDR is still not widely disseminated in Brazil7. Considering that CP is the most common cause of physical disability in childhood and that spasticity represents a relevant functional limitation in this population, the scarcity of national reports with longitudinal follow-up makes it difficult to understand the functional impacts of SDR when associated with physiotherapeutic rehabilitation programs, as well as to analyze contextual factors that influence these outcomes7. In this sense, case reports become relevant, as they allow an in-depth analysis of individual functional evolution, contributing to clinical practice and to the discussion about expanding access to this intervention in the Brazilian context.
Thus, the aim of this report was to describe the changes in gross motor function and mobility of a child with bilateral spastic cerebral palsy, diplegic type, from the Zona da Mata region of Minas Gerais, before and after Selective Dorsal Rhizotomy, over 18 months of follow-up, considering functional aspects, physiotherapeutic rehabilitation process, and contextual factors associated with the case.
2. Case Report
2.1 Study design and ethical aspects
This is a retrospective observational study, approved by the Research Ethics Committee of the University Hospital of Juiz de Fora (Hospital Universitário de Juiz de Fora - HU-UFJF) (CAAE: 09581119.1.0000.5133). The Informed Consent Form and the authorization for image use were signed by the child's mother.
2.2 Participant
The participant is a male child, collaborative, communicative, and cheerful, currently 5 years old, diagnosed with bilateral spastic cerebral palsy, diplegic type, classified as level III in the Gross Motor Function Classification System (GMFCS). In the preoperative period, he presented bilateral spasticity, assessed using the Modified Ashworth Scale, with a score of 1 for knee extensors and flexors, plantar flexors, toe flexors, and hip flexors, and a score of 3 for hip abductors. He lives with his parents in a spacious, privately owned home adapted with handrails, which facilitates his mobility. The child attends a local daycare school and receives daily support from a teacher and an assistant to facilitate his mobility, participation in activities, and interaction with peers.
2.3 Interventions
At 3 years and 8 months of age, the study participant underwent Lumbar Selective Dorsal Rhizotomy at the conus medullaris, with multimodal monitoring conducted by a neurophysiologist and a neurofunctional physiotherapist. Simultaneously, an orthopedic correction with bilateral triceps surae lengthening was performed. The main objectives were reduction of spasticity, biomechanical alignment of the feet, improvement in gait quality, and reduction of functional limitations resulting from spasticity.
The surgery was performed at a private hospital in Teresina, Piauí, Brazil, in March 2023. This scenario was only possible due to the family’s dedication, who organized a fundraising campaign to cover the costs of the procedure.
The immediate postoperative protocol, initiated seven days after surgery, began in Teresina at the Rizo Institute, with intensive physiotherapy, comprising forty daily therapy sessions. During the first four weeks, the patient remained with short leg casts and restricted weight-bearing on the lower limbs. After cast removal, weight-bearing was gradually introduced over the following two weeks.
In May 2023, the child began follow-up at the Physiotherapy Outpatient Clinic of the University Hospital of the Federal University of Juiz de Fora (HU-UFJF), where the assessment and therapeutic approach follow the biopsychosocial model of the International Classification of Functioning, Disability and Health (ICF). Outpatient sessions occurred three times per week, reaching an attendance rate of 90%, according to hospital medical records. In addition, the child received home-based therapy twice a week and therapy at daycare once a week. The home environment included therapeutic resources used for training, such as parallel bars, a treadmill, and a Swiss ball. The family’s dedication was evidenced by the active involvement of the parents during therapy sessions, participation in clinical decision-making, and adherence to therapeutic training and guidance carried out at home.
Figure 1 describes the participant at the beginning of treatment, based on the biopsychosocial model of the ICF.
Figure 1. Framework of the International Classification of Functioning, Disability and Health (ICF) of the participant
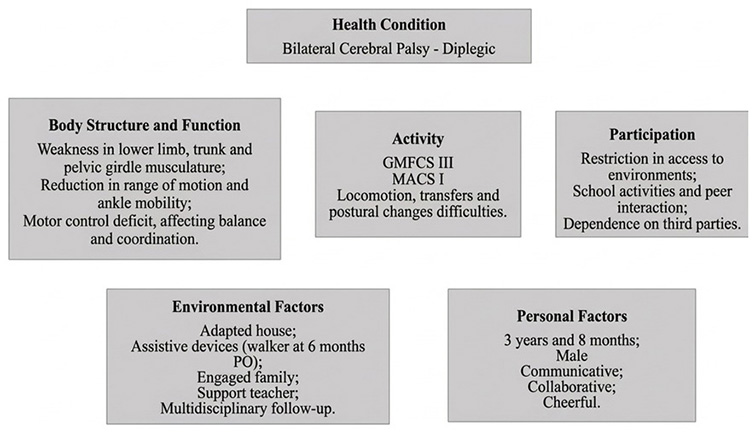
According to the electronic medical records of the hospital (AGHU system), the physiotherapeutic assessment performed after surgery indicated ankle dorsiflexion deficit, weakness in the lower limbs, trunk, and pelvic girdle, which compromised balance and motor coordination when attempting to stand and walk. These impairments limited his independence in daily activities, such as standing, walking with support, and performing transfers, leading him to remain seated most of the time. At school, he faced difficulties interacting and participating in activities, being dependent on a wheelchair for mobility. The assistance of the teacher was essential for movement between environments. This situation improved after strength gains in the lower limbs, which enabled the acquisition of a posterior walker for gait, six months after surgery.
The treatment plan was based on goal attainment and focused on task-oriented training relevant to each stage, always with the active participation of the child. At intervals of approximately three months, the objectives and adaptations were adjusted according to the patient’s new demands. The therapeutic plan gradually incorporated strengthening of the lower limbs and trunk, acquisition of balance in the standing posture, supported gait training, and functional transfers, in a progressive and sequential manner. The follow-up lasted 18 months, with evaluations conducted at intervals of approximately three months.
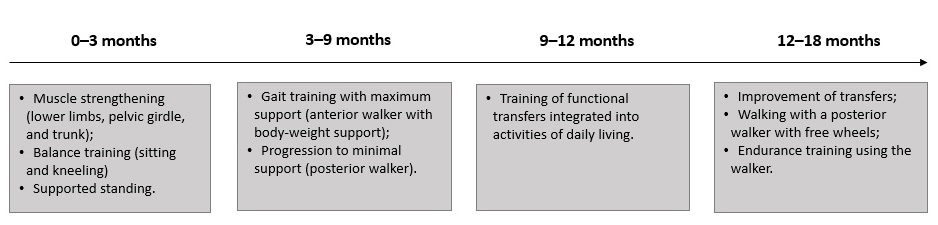
During the first trimester, interventions were directed toward strengthening the lower limbs, pelvic girdle muscles, spinal extensors, abdominal muscles, as well as improving balance in sitting and kneeling positions and supported standing posture. Between three and six months, gait training was initiated, beginning with maximum support (an anterior walker adapted with body-weight support) and progressively reducing assistance until minimal support (posterior walker) was achieved. Between nine and twelve months, functional transfer training integrated into activities of daily living was initiated. Finally, the last six months were directed toward refining transfers, independent walking using a posterior walker with free wheels, and improving physical endurance, with a progressive increase in the daily time spent walking with the walker. The physiotherapeutic interventions carried out throughout this period are chronologically summarized in figure 2.
Figure 2. Chronological overview of the therapeutic plan during the postoperative period
2.4 Outcome measures
The primary outcome of the study was to evaluate changes in motor skills throughout the postoperative follow-up. To monitor the progression of surgical intervention and physiotherapeutic rehabilitation, the participant was assessed in the preoperative period and re-evaluated every three months using the Gross Motor Function Measure (GMFM-66), an instrument that quantitatively describes the motor capacity of children with cerebral palsy8.
The Modified Ashworth Scale was used to quantify changes in the degree of spasticity before and after surgery9.
Expected Natural Evolution (ENE) was used to estimate the predicted change in GMFM-66 scores at each assessment, allowing analysis of whether the participant’s scores exceeded those expected for natural motor development, thereby contributing to the interpretation of the impact of the surgical intervention associated with physiotherapeutic rehabilitation10.
2.5 Data analysis
A descriptive analysis of the case was conducted, reporting the stages of treatment and the functional evolution based on GMFM-66 scores, which were applied before surgery and at 3, 6, 9, 12, and 18 months after surgical intervention. The data for this study, including assessments and treatment plan, were extracted from the hospital’s electronic medical records, covering the period from the preoperative stage to 18 months postoperatively.
The total GMFM-66 scores were analyzed using the Gross Motor Ability Estimator software (GMAE-3), which also enabled the calculation of the Expected Natural Evolution (ENE) based on the participant’s age, the GMFM score obtained, the interval between assessments in months, and the changes achieved at each evaluation10.
The statistical analysis considered the differences between the intervention periods to be significant when the variation in total GMFM-66 score exceeded the upper limit of the 95% confidence interval (p<0.05) in relation to the previous assessment10.
3. Results
Table 1 presents the GMFM-66 test scores, the percentage changes, the 95% confidence interval, and variation in points obtained in each assessment compared to the preoperative evaluation. In addition, it shows the expected change in points based on the Expected Natural Evolution (ENE) and the actual variation observed in the GMFM-ER10. The change score values were significantly higher than the expected change based on natural evolution (p<0.05).
Table 1. GMFM-66 scores and percentage changes
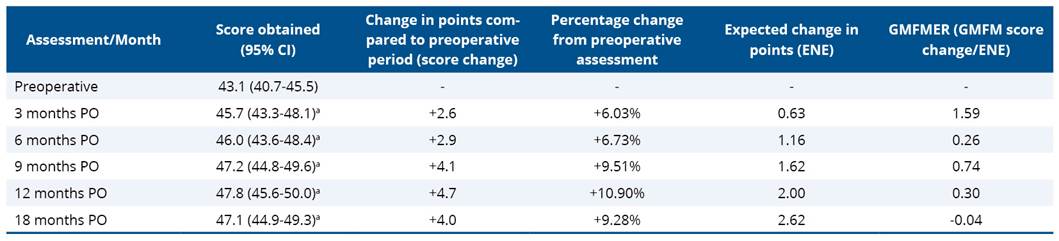
aSignificant increase in the test value compared to preoperative period; ENE: Expected Natural Evolution; GMFM score change: change in points compared to the preoperative period; GMFMER: relationship between the observed change in points and expected natural evolution; CI: Confidence Interval; PO: postoperative.
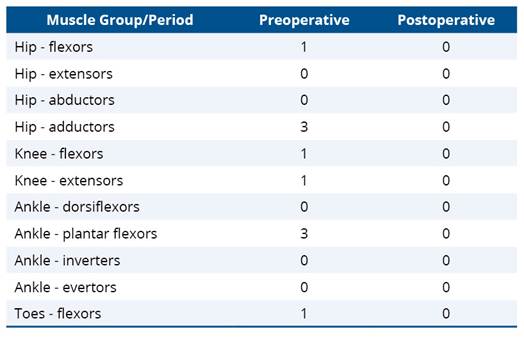
Table 2 presents the scores of the Modified Ashworth Scale in the preoperative and postoperative periods.
Table 2. Modified Ashworth Scale scores in the preoperative and postoperative periods
4. Implications
This case report demonstrated a progressive improvement in the functioning of a child with diplegic cerebral palsy who underwent Selective Dorsal Rhizotomy (SDR), associated with a structured physiotherapeutic rehabilitation program over 18 months of postoperative follow-up. The main findings include reduction of spasticity after SDR, functional gains greater than the expected natural evolution, and the acquisition of supported gait and functional transfers, measured using a standardized instrument to assess gross motor function in children with cerebral palsy. In addition, the findings highlight the integrated role of surgical intervention and physiotherapy in the rehabilitation process.
The reduction in spasticity was associated with improvements in motor function, since after the surgical intervention all variations in scores compared to the preoperative period were higher than the changes predicted by the expected natural evolution. These results corroborate evidence indicating that children classified as GMFCS level III who undergo SDR tend to achieve greater gains than those observed in the natural course of cerebral palsy, in which an early functional plateau followed by progressive decline is commonly observed11. Thus, this case report highlights the clinical relevance of SDR as a strategy capable of modifying the expected functional trajectory in this population.
Regarding the temporal trajectory of the assessments, gains were observed up to 12 months, with the highest score occurring in the first 3 months, a period during which the participant acquired skills such as sitting trunk control and kneeling posture, which had previously been limited by spasticity of the lower limbs. After this period, the scores showed slight fluctuations. The literature describes that most functional gains after SDR tend to occur within the first 12 postoperative months, followed by a period of stabilization of motor function, consistent with the prognostic curves of cerebral palsy progression11. This pattern was also observed in the present case when comparing the assessments performed at 12 and 18 months of follow-up.
The success observed in this case can be understood in light of a set of favorable factors. The child’s age, combined with his functional classification, indicated a period of greater potential for motor gains, as described in the literature for children with spastic diplegia who undergo SDR between 3 and 8 years of age12. In addition, the orthopedic correction was performed at a stage considered ideal for patients classified as GMFCS level III, contributing to improved postural alignment and greater gait efficiency13. The combination of these factors, together with a structured physiotherapeutic rehabilitation plan, helps explain the functional gains observed.
In addition to the surgical aspects, contextual factors also appear to have positively influenced the observed outcomes. Notable among these were the active involvement of the family in defining a therapeutic plan with realistic goals, adaptations made in the home environment to facilitate the child’s daily activities and independence, as well as the promotion of participation in different social environments. These elements are recognized as facilitators of functioning and quality of life in children with cerebral palsy, according to the ICF model14.
From a clinical perspective, this case report reinforces the importance of the integration between SDR and physiotherapeutic follow-up, before, during, and after the surgical procedure. For physiotherapists and families, the findings highlight the importance of individualized therapeutic planning, with longitudinal monitoring and adaptation of interventions according to the child’s needs, focusing on functioning, context, and participation7.
Because this is a case report, the generalizability of the findings is limited, since the results reflect the experience of a single participant. The absence of a comparison group and the observational nature of the study limit broader causal inferences about the effects of the interventions. Furthermore, the exclusion of additional instrumental measures, such as quantitative gait analysis or kinematic and kinetic assessments, restricts a more detailed understanding of the biomechanical mechanisms underlying the observed functional gains. Contextual factors, such as family involvement, adaptations in the home environment, adherence to the rehabilitation program, and the child's active participation in therapies and in different social contexts, may also have positively influenced the outcomes. Even so, the use of standardized instruments for children with CP and the detailed follow-up period allows for a deeper understanding of this child's functional evolution after SDR, contributing to clinical practice and future investigations with more robust designs.
5. Conclusion
In the context of this case report, Selective Dorsal Rhizotomy (SDR) demonstrated its potential for reducing spasticity and improving gross motor function in a child with cerebral palsy. Performing the surgery at a clinically favorable stage, combined with evidence-based physiotherapeutic rehabilitation, contributed to the functional evolution observed. The active involvement of the child and family in this process is also noteworthy, reinforcing the value of an integrated and family-centered approach that considers the contextual factors of the child’s daily life. Given that this is a case report, the findings should be interpreted with caution. Further studies with larger samples and more robust study designs are needed to expand the understanding of the effects of SDR associated with physiotherapeutic rehabilitation.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Hägglund G, Hollung SJ, Ahonen M, Andersen GL, Eggertsdóttir G, Gaston MS, et al. Treatment of spasticity in children and adolescents with cerebral palsy in Northern Europe: a CP-North registry study. BMC Neurol. 2021;21(1):276. https://doi.org/10.1186/s12883-021-02289-3
2. Paul S, Nahar A, Bhagawati M, Kunwar AJ. A review on recent advances of cerebral palsy. Oxid Med Cell Longev. 2022:1–20. https://doi.org/10.1155/2022/2622310
3. Dan B, Rosenbaum P, Carr L, Gough M, Coughlan J, Nweke N. Proposed updated description of cerebral palsy. Dev Med Child Neurol. 2025;67(6):700-9. https://doi.org/10.1111/dmcn.16274
4. Kudva A, Abraham ME, Gold J, Patel NA, Gendreau JL, Herschman Y, et al. Intrathecal baclofen, selective dorsal rhizotomy, and extracorporeal shockwave therapy for the treatment of spasticity in cerebral palsy: a systematic review. Neurosurg Rev. 2021;44(6):3209-28. https://doi.org/10.1007/s10143-021-01550-0
5. Romei M, Oudenhoven LM, Van Schie PEM, Van Ouwerkerk WJR, Van der Krogt MM, Buizer AI. Evolution of gait in adolescents and young adults with spastic diplegia after selective dorsal rhizotomy in childhood: a 10-year follow-up study. Gait Posture. 2018;64:108–13. https://doi.org/10.1016/j.gaitpost.2018.06.002
6. Alves LFC, Almeida IV, Naves RVG, Oliveira AJM. Short- and long-term effects of selective dorsal rhizotomy in the treatment of spasticity. Braz J Hea Rev. 2020;3(6):18888–93. https://doi.org/10.34119/bjhrv3n6-275
7. Nicolini-Panisson RD, Tedesco AP, Folle MR, Donadio MVF. Selective dorsal rhizotomy in cerebral palsy: indication criteria and postoperative physiotherapeutic rehabilitation protocols. Rev Paul Pediatr. 2018;36(1):100–8. https://doi.org/10.1590/1984-0462/;2018;36;1;00005
8. Russell DJ, Wright M, Rosenbaum PL, Avery LM. Gross Motor Function Measure (GMFM-66 & GMFM-88) user’s manual. 3rd ed. London: Mac Keith Press; 2021.
9. Harb A, Margetis K, Kishner S. Modified Ashworth Scale. In: StatPearls. Treasure Island: StatPearls Publishing; 2025 [cited 2026 fev. 10]. Cited: PMID: 32119459.
10. Marois P, Marois M, Pouliot-Laforte A, Vanasse M, Lambert J, Ballaz L. Gross Motor Function Measure Evolution Ratio: use as a control for natural progression in cerebral palsy. Arch Phys Med Rehabil. 2016;97(5):807–14 https://doi.org/10.1016/j.apmr.2015.07.024
11. Iorio-Morin C, Yap R, Dudley RWR, Poulin C, Cantin MA, Benaroch TE, et al. Selective dorsal root rhizotomy for spastic cerebral palsy: a longitudinal case-control analysis of functional outcome. Neurosurgery. 2020;87(2):186-92. https://doi.org/10.1093/neuros/nyz422
12. Kim HS, Steinbok P, Wickenheiser D. Predictors of poor outcome after selective dorsal rhizotomy in treatment of spastic cerebral palsy. Childs Nerv Syst. 2006;22(1):60–6. https://doi.org/10.1007/s00381-005-1160-2
13. Heinen F, Desloovere K, Schroeder AS, Berweck S, Borggraefe I, van Campenhout A, et al. The updated European consensus 2009 on the use of botulinum toxin for children with cerebral palsy. Eur J Paediatr Neurol. 2010;14(1):45–66. https://doi.org/10.1016/j.ejpn.2009.09.005
14. Chagas PSC, Magalhães EDD, Sousa Junior RR, Romeros ACSF, Palisano RJ, Leite HR, et al. Desenvolvimento de crianças, adolescentes e jovens adultos com Paralisia Cerebral de acordo com a CIF? Uma revisão do escopo. Dev Med Child Neurol. 2023;65(6):e61-9. https://doi.org/10.1111/dmcn.15487
