Original article
Association between physical fitness, fundamental motor competency, and joint mobility among school-going children in Moodbidri town, South India / Associação de aptidão física, competência motora fundamental e mobilidade articular entre crianças em idade escolar na cidade de Moodbidri, sul da Índia
Kshama Shetty1 (https://orcid.org/0000-0003-1479-4983)
Hariharasudhan Ravichandran2 (https://orcid.org/0000-0002-0703-9675)
Soumya Ranjan Sahoo3 (https://orcid.org/0009-0008-6600-4086)
Noble Vavachan4 (https://orcid.org/0009-0007-5188-2655)
Swapnika Sanjay Satam5 (https://orcid.org/0009-0008-9253-0725)
Balamurugan Janakiraman6 (https://orcid.org/0000-0003-3866-9351)
1 Corresponding contact. Meenakshi Academy of Higher Education and Research (Chennai). Tamil Nadu, India. [email protected]
2,3,5Alva’s College of Physiotherapy and Research Centre (Moodbidri). Karnataka, India.
4JSS College of Physiotherapy (Mysore). Karnataka, India.
6SRM Institute of Science and Technology (Chennai). Tamil Nadu, India.
ABSTRACT | BACKGROUND: In typically developing children, physical fitness and fundamental motor skills are closely related and develop in tandem. Whether the strength of this relationship differs in children with generalized joint hypermobility remains unclear. OBJECTIVE: To compare the associations between physical fitness components and fundamental motor skill competency in children with and without generalized joint hypermobility. METHODS: This cross-sectional study included 313 school-going children recruited from eight school clusters in Moodbidri, South India. Ethical approval was obtained, and informed consent was secured from school authorities and parents. Physical fitness and fundamental motor skills were assessed over two consecutive days. Physical fitness measures included speed, endurance, flexibility, balance, muscular strength, power and coordination. Fundamental motor skills were evaluated using the locomotor and object control subscales of the Test of Gross Motor Development-2 (TGMD-2). RESULTS: Children with and without generalized joint hypermobility were comparable in age and anthropometric characteristics. Significant differences were observed between groups in several physical fitness components and fundamental motor skill proficiency (p < 0.05). Spearman correlation analyses demonstrated significant associations between selected physical fitness measures and fundamental motor skills in both groups, with Fisher’s r-to-z transformation indicating differences in the strength of these associations between hypermobile and non-hypermobile children. CONCLUSION: The strength of associations between physical fitness components and fundamental motor skill proficiency differs between children with generalized joint hypermobility and those with normal joint mobility, highlighting joint mobility status as an important consideration when interpreting fitness–motor skill relationships in school-aged children.
KEYWORDS: Motor Skills. Physical Fitness. Joint Hypermobility Syndrome. Children.
RESUMO | CONTEXTO: Em crianças com desenvolvimento típico, a aptidão física e as habilidades motoras fundamentais estão intimamente relacionadas e se desenvolvem em conjunto. Resta saber se a intensidade dessa relação difere em crianças com hipermobilidade articular generalizada. OBJETIVO: Comparar as associações entre os componentes da aptidão física e a competência em habilidades motoras fundamentais em crianças com e sem hipermobilidade articular generalizada. MÉTODOS: Este estudo transversal incluiu 313 crianças em idade escolar, recrutadas em oito grupos de escolas do projeto Moodbidri, no sul da Índia. A aprovação ética foi obtida e o consentimento informado foi garantido pelas autoridades escolares e pelos pais. A aptidão física e as habilidades motoras fundamentais foram avaliadas em dois dias consecutivos. As medidas de aptidão física incluíram velocidade, resistência, flexibilidade, equilíbrio, força muscular, potência e coordenação. As habilidades motoras fundamentais foram avaliadas utilizando as subescalas de locomoção e controle de objetos do Teste de Desenvolvimento Motor Global-2 (TGMD-2). RESULTADOS: Crianças com e sem hipermobilidade articular generalizada apresentaram idades e características antropométricas comparáveis. Diferenças significativas foram observadas entre os grupos em diversos componentes da aptidão física e na proficiência em habilidades motoras fundamentais (p < 0,05). As análises de correlação de Spearman demonstraram associações significativas entre medidas selecionadas de aptidão física e habilidades motoras fundamentais em ambos os grupos, com a transformação r-para-z de Fisher indicando diferenças na força dessas associações entre crianças hipermóveis e não hipermóveis. CONCLUSÃO: A força das associações entre os componentes da aptidão física e a proficiência em habilidades motoras fundamentais difere entre crianças com hipermobilidade articular generalizada e aquelas com mobilidade articular normal, destacando o estado da mobilidade articular como uma consideração importante na interpretação das relações entre aptidão física e habilidades motoras em crianças em idade escolar.
PALAVRAS-CHAVE: Habilidades Motoras. Aptidão Física. Síndrome da Hipermobilidade Articular. Crianças.
How to cite this article: Shetty K, Ravichandran H, Sahoo SR, Vavachan N, Satam SS, Janakiraman B. Association between physical fitness, fundamental motor competency, and joint mobility among school-going children in Moodbidri town, South India. J Physiother Res. 2026;16:e6493. https://doi.org/10.17267/2238-2704rpf.2026.e6493
Submitted Oct. 5, 2025, Accepted Dec. 19, 2025, Published Mar. 18, 2026
J. Physiother. Res., Salvador, 2026;16:e6493
https://doi.org/10.17267/2238-2704rpf.2026.e6493
ISSN: 2238-2704
Assigned editor: Juliana Goulardins
1. Introduction
Fundamental motor skills, including locomotor and object control skills, are the building blocks for more complex and specialized movements used in play, physical activity, and sports1. Foundational movements such as running, jumping, throwing, and catching contribute to children’s physical development and future participation in physical activity2. Building fundamental motor skills during childhood is crucial for developing motor competence and promoting participation in physical activity and overall health3. Equally important is physical fitness; beyond being a health indicator, its components, such as muscular strength, endurance, flexibility, and cardio-respiratory capacity, are essential for executing motor skills proficiency4. Gao et al.5 reported that children with higher fitness levels tend to perform better in motor skill tasks, suggesting a strong interdependency between these two constructs.
The concept of physical literacy provides a broader framework for understanding how physical fitness and fundamental motor skills develop and interact during childhood. Physical literacy encompasses physical competence, motivation, confidence, knowledge, and understanding that enable individuals to engage in physical activity across the lifespan. Fundamental motor skills represent a core component of physical competence within physical literacy, forming the foundation for children’s participation in play, sport, and physical activity. When fundamental motor skills and physical fitness develop harmoniously, they support sustained engagement in movement and contribute to a positive developmental trajectory toward lifelong physical activity. Conversely, impairments in physical competence, such as those arising from altered joint mobility, may disrupt physical literacy development by limiting movement efficiency, confidence, and engagement in physical activity.
Although the benefits of developing fundamental motor skills and physical fitness are well-established, comparatively less attention has been given to the biomechanical factors that enable proficient movement. Optimal joint mobility is required for efficient movement6. In children with normal joint mobility, research consistently demonstrates a positive association between fundamental motor skill proficiency and various components of physical fitness7. Earlier, assumptions suggested that joint hypomobility was a major risk factor for sustaining musculoskeletal injuries. However, more recent studies8,9 have reported contradictory findings, indicating that hypomobility does not necessarily increase injury risk, whereas hypermobility may be associated with a higher risk.
Generalized joint hypermobility is reported to occur in 10–20% of children10. While often asymptomatic, it may also be associated with musculoskeletal discomfort and delayed motor development11. The literature presents inconclusive evidence12,13 regarding how joint hypermobility is related to physical fitness performance. Black et al.12 reported that hypermobile children demonstrate reduced muscle strength and endurance, which may be associated with poor performance on physical tasks. Other studies13,14 have proposed that increased joint laxity may contribute to a "mechanical insufficiency," making physical activity more demanding and fatiguing. Additionally, de Koning et al.15 found that children with joint hypermobility often experience difficulty competing in physical play and sporting activities. Subclinical impairments in joint stability, proprioception, and postural control in children with hypermobility may also be related to challenges in the development of fundamental motor skills; however, empirical evidence supporting this relationship remains limited.
Despite this body of literature, it remains unclear whether the strength of the relationship between physical fitness and fundamental motor skills differs between children with and without generalised joint hypermobility. Understanding whether hypermobility status is associated with differences in this relationship is important, as alterations in the coordination between physical fitness and motor skill development may compromise physical literacy and potentially reduce lifelong participation in physical activity. According to the International Classification of Functioning, Disability and Health (ICF), human functioning is conceptualised across multiple interacting domains, including Body Structures and Functions, Activities, Participation, and contextual factors. The present study primarily focuses on the Body structures and Body functions components of the ICF framework, as it examines joint mobility characteristics, physical fitness attributes, and fundamental motor skill proficiency. Although fundamental motor skills relate to activity-level performance, the assessments used in this study were performance-based tests rather than measures of participation or habitual physical activity. By addressing this gap, the present study aims to contribute meaningful insights into paediatric motor development that may assist clinicians, educators, and therapists in tailoring early interventions, physical education programs, and therapeutic approaches based on individual needs. Therefore, this cross-sectional study aims to compare the relationship between physical fitness and fundamental motor skills representing body functions and activity related performance between children with and without generalized joint hypermobility.
2. Method
2.1 Ethical committee and guidelines
Approval for this correlational cross-sectional study was obtained from the Institutional Ethical Committee of Alva’s College of Physiotherapy and Research Centre, Moodbidri, Dakshina Kannada, Karnataka. The design of this study protocol adheres to the STROBE guidelines for observational studies, and it is registered in the Clinical Trial Registry of India (CTRI/2024/07/070333) accordingly.
2.2 Sample size estimation
This sample size estimation was performed with G*power statistical software (version 3.1.9.4). The study sample size was calculated through a power analysis16 that showed that a total sample size of 88 per group was needed for a medium effect size (d = 0.5), at a power 95%, while alpha is set at 5% with an allocation ratio of 1.
2.3 Sample source, study setting and sampling technique
There are 8 school clusters Moodbidri, which include the Moodbidri main cluster, Handelu cluster, Iruvailu cluster, Jyothi Nagar cluster, Kallamundkur cluster, Padukonaje cluster, Borugudde cluster, and Beluvai cluster. The study protocol was explained to the Principal and the Physical Education teacher of schools from these clusters. A recruitment flyer was posted on school notice boards, inviting parents of children aged 7 to 11 years to contact the investigators if they are interested in having their child participate. The physical fitness and fundamental motor skill competency tests were conducted at the outdoor sporting facilities of Alva’s Sports Academy in Moodbidri, Karnataka. Informed parental consent was obtained from the legal parent or guardian for children participating in the research. Through non-probability and convenience sampling methods, children were enrolled in the present study.
2.4 Selection criteria
Both boys and girls aged 7 to 11 years were included in this study. Joint mobility status was screened using the Beighton scoring criteria17, which assesses the mobility of the spine and the bilateral little finger, elbow, knee, and thumb. Children were classified as having normal joint mobility (Beighton scores of 0 to 5) or hypermobile joints (Beighton scores of 6 to 9). Exclusion criteria included musculoskeletal pain, deformities, cardiovascular risks, respiratory pathologies, neurocognitive disorders, other known systemic illnesses, any motor or sensory impairments, and parents unwilling to provide consent.
2.5 Data collection
Physical fitness tests and Fundamental motor skill tasks (from TGMD-2) were conducted in children fulfilling the selection criteria. Four senior Physiotherapists with Sports Physiotherapy qualifications and specialized in administering Physical fitness and Fundamental motor skill tests were engaged for data collection. Habitual physical activity levels were not assessed in the present study.
2.5.1 Physical fitness tests
Two senior physiotherapists conducted the following physical fitness tests on the children: the 10 x 5m shuttle run, 600m endurance run, sit and reach, consecutive both feet jumps, flamingo balance, curl-ups, hand grip, vertical jump, and throwing a tennis ball. Most of these physical fitness tests are components of the Sports Authority of India's Khelo India fitness test for school children. This is the rationale for their inclusion in the study. The psychometric properties of these tests have been established in the literature for this age group18.
Speed and Agility: A 10x5m shuttle run was conducted to measure speed and agility. Children ran between two markers placed 5 meters apart, completing ten segments for a total distance of 50 meters. The time was recorded using timing gates19.
Cardiovascular Endurance: A 600m endurance run was used to assess cardiovascular fitness. Children were instructed to complete the distance in the shortest time possible19.
Flexibility: A standard sit-and-reach box measured lower back and hamstring flexibility. The child sat with legs extended and feet against the box, reached forward as far as possible, and held the position for one or two seconds. The score was recorded to the nearest centimeter19.
Lower Extremity Coordination: The Consecutive both feet jump test assessed lower extremity coordination. The child jumped forward with both feet together from a standing start. The distance between two jumps was measured in feet19.
Balance: The flamingo balance test assessed the ability to balance on one leg for one minute. The number of times the child lost their balance was counted19.
Abdominal Strength and Endurance: The curl-up test measured abdominal muscle strength and endurance. The child performed as many curl-ups as possible in one minute, with knees flexed, feet flat, and arms folded across the chest19.
Hand Grip Strength: A Jamar dynamometer, used in accordance with the guidelines of the American Society of Hand Therapists, measured hand grip strength. The child performed three trials while seated with the shoulder adducted and neutrally rotated, elbow flexed at 900, wrist at 00 to 300 extension, and 00 to 150 ulnar deviation. The maximum force from the three trials was recorded19.
Explosive Power: A vertical jump test using a Vertec device estimated explosive power. Standing reach height was measured, and the child then performed three maximal vertical jumps, attempting to hit the flags with their fingertips. The difference between the maximum jump height and the standing reach height was recorded in cm19.
Upper Limb Strength and Power: Throwing a tennis ball for distance (measured in meters) estimated upper limb strength and explosive power19.
2.5.2 Fundamental motor skill
The Test of Gross Motor Development-2 (TGMD-2) was used to assess the Fundamental Motor Skill (FMS) performance of children in this study20.
As a standardized, norm-referenced tool, the TGMD-2 measures gross motor skills through its locomotor and object control subtests. Its validity and reliability have been widely established in pediatric populations21.
2.6 Data analysis
Data were prepared for analysis in SPSS (IBM, version 27.0.1) through editing (field and central), coding, categorization, cleaning, and tabulation. Baseline characteristics for children with normal and hypermobile joints were compared using independent t-tests. Normality of the data was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests. As the data were not normally distributed, the Mann-Whitney U test was used for group comparisons, and Spearman's rank correlation was used to assess the relationship between physical fitness and fundamental motor skill performance. Fisher's r-to-z transformation was performed to test whether the correlation coefficients differed significantly between the normal and hypermobility groups. Given the cross-sectional observational design, analyses were limited to group comparisons, association testing, and comparison of correlation strengths, without inference of causal relationships.
3. Results
3.1 Demographic characteristics
The study included 209 children with normal joint mobility and 104 children with generalized joint hypermobility. The mean age for the overall cohort was 8.12 years, with no significant difference observed between the hypermobile and non-hypermobile groups. Baseline anthropometric characteristics, including height, weight, and body mass index (BMI), were also similar between the groups. As BMI does not distinguish between muscle and fat mass, estimates of body fat percentage and waist-hip ratio were additionally included in the demographic comparison. These measures were also similar across both groups (Table 1).
Physical fitness and TGMD-2 data, specifically locomotor and object control scores, were collected for the study. Normality tests (Kolmogorov-Smirnov and Shapiro-Wilk tests; p < 0.001) indicated that the data were not normally distributed. Therefore, the Mann-Whitney U test was used to analyze differences in these scores between children with normal joint mobility and those with generalized joint hypermobility.
Table 1. Demographic and baseline anthropometric characteristics of children with and without generalized joint hypermobility
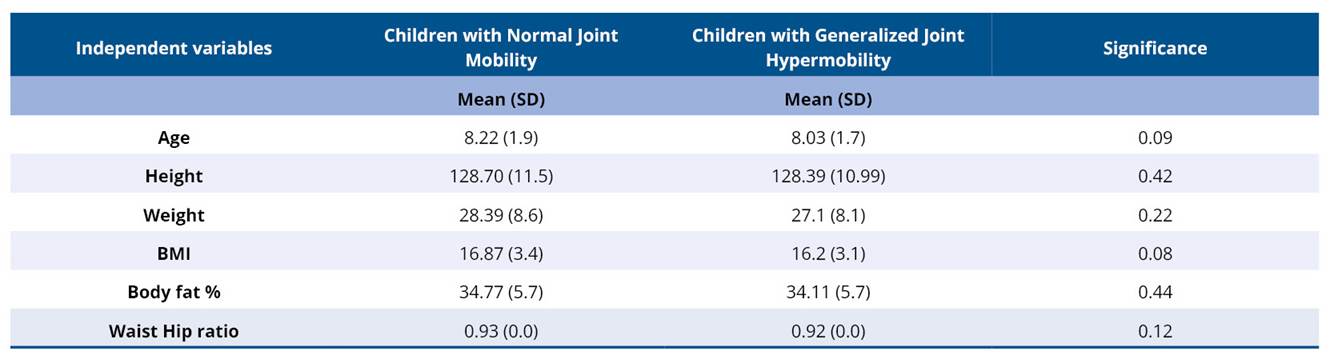
* significant if p < 0.05.
Table 2. Mann Whitney U test for Physical fitness variables among children with and without generalised joint hypermobility
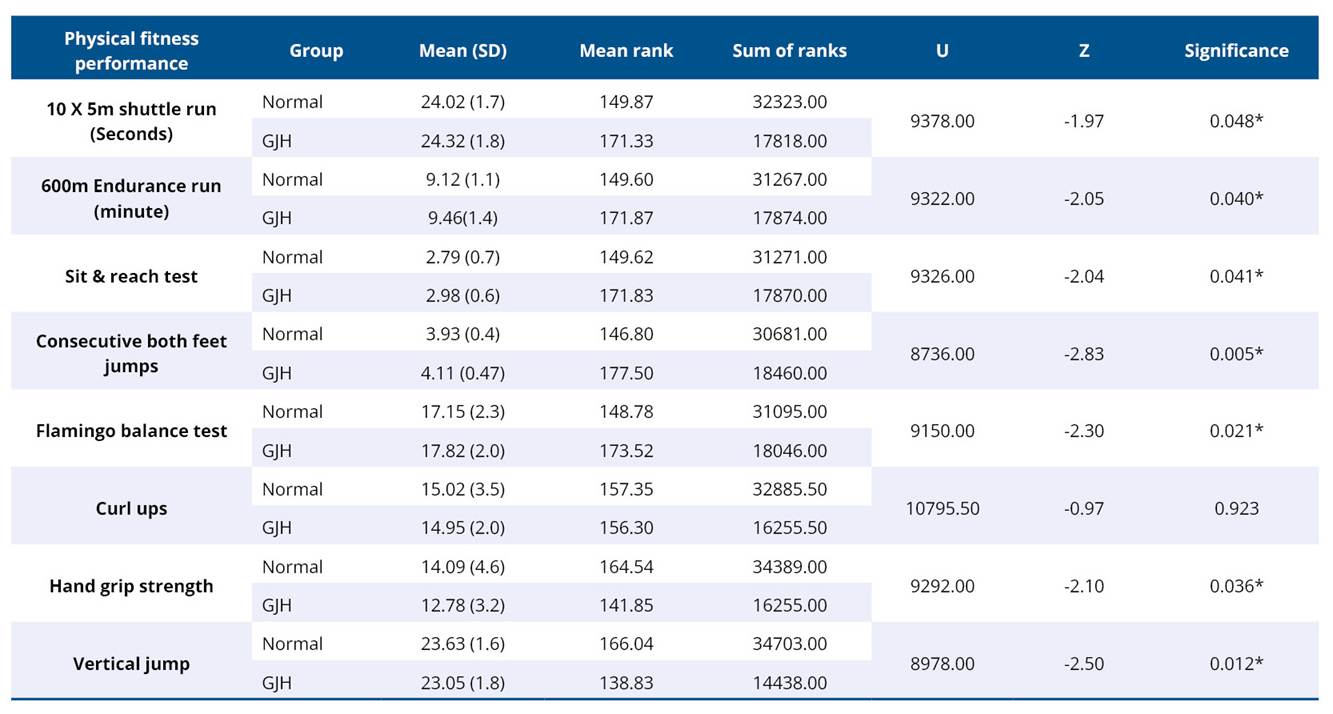
* significant if p < 0.05.
Table 3. Mann Whitney U test for fundamental motor skill variables among children with and without generalised joint hypermobility
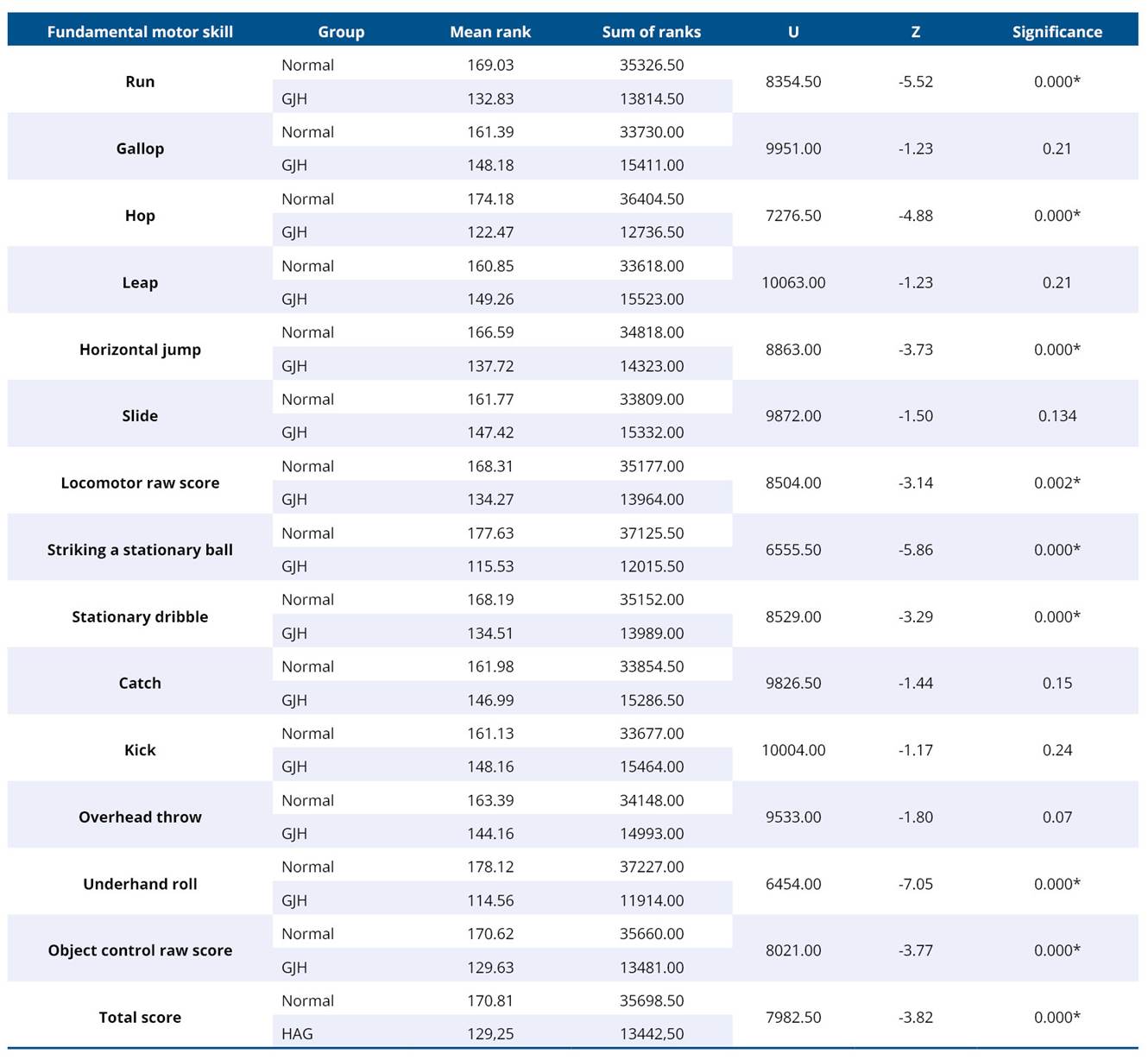
* significant if p < 0.05.
Table 4. Spearman's rho correlation coefficients (r) for fundamental motor skill and physical fitness variables in children with normal joint mobility and children with generalized joint hypermobility

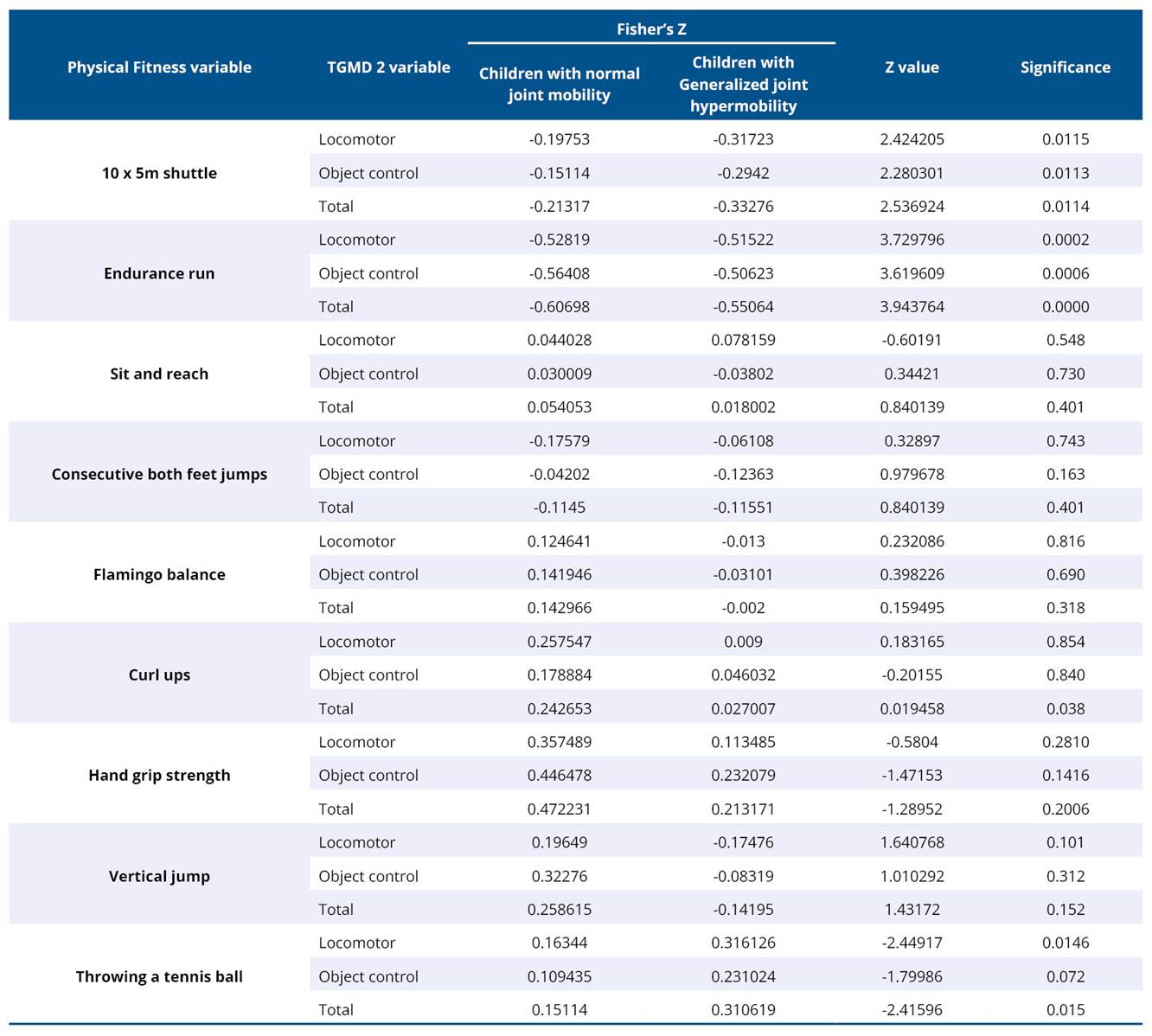
Table 5. Comparison of correlation coefficients between normal and hypermobile children using Fisher's z-test
4. Discussion
The primary objective of this study was to examine the correlation between physical fitness components and fundamental motor skill proficiency by comparing children with normal joint mobility and those with generalized joint hypermobility. The results confirm two critical findings. First, a significant association exists between the 10 x 5m shuttle run and the 600m endurance run component of physical fitness, and fundamental motor skill mastery in both groups, supporting the notion that physical fitness facilitates motor competence development in typically developing children. Second, and more importantly, the strength of this association differed significantly between children with normal joint mobility and those with generalised joint hypermobility.
Interpreting these findings within the ICF framework, the present results primarily reflect interactions at the level of Body Functions and Body Structures, with outcomes measured through performance-based indicators of activity capacity. The observed differences between children with normal joint mobility and those with generalized joint hypermobility highlight how impairments at the structural and functional level such as joint laxity and neuromuscular control deficits can influence movement performance. However, these findings do not necessarily capture participation-level restrictions or real-world physical activity engagement.
When interpreted through the lens of physical literacy, the findings suggest that children with generalized joint hypermobility may experience challenges in developing physical competence, a central domain of physical literacy. Although physical fitness and fundamental motor skills were associated in both groups, the weaker relationships observed in hypermobile children indicate that structural and neuromuscular constraints may limit efficient skill acquisition. Over time this may influence motivation, confidence, and sustained engagement in physical activity key components necessary for the development of physical literacy.
4.1 Association between physical fitness and fundamental motor skill proficiency
Children, irrespective of their joint mobility status, who demonstrated better performance in 10 x 5m shuttle run and 600m endurance run achieved higher scores on the locomotor subscale and total score of the Fundamental Motor Skill Proficiency Test. This indicates a significant statistical association between physical fitness and fundamental motor skill proficiency. This relationship was observed in both children with normal joint mobility and those with generalized joint hypermobility, aligning with the “motor proficiency barrier model”22, which posits that adequate physical fitness, particularly neuromuscular function and aerobic capacity is a prerequisite for the development of fundamental motor skills.
The 10 x 5m shuttle run assesses speed, agility, and rapid changes of direction, directly reflecting the mastery of dynamic balance and locomotor control. Similarly, the 600m run, which evaluates cardiorespiratory endurance, may support fundamental motor skill mastery by providing the sustained energy required for repeated practice, thereby promoting greater physical activity exposure and skill consolidation. These findings are consistent with the developmental model proposed by Bardid et al.23, which emphasizes a dynamic and reciprocal relationship between motor competence and physical fitness across childhood. According to this model, children with higher motor competence are more likely to engage in physical activity, which further enhances fitness, creating a positive feedback loop.
The absence of significant correlations between fitness tests (sit-and-reach test, consecutive both-feet jumps, flamingo balance test, vertical jump test, curl-ups, handgrip strength test, and throwing a tennis ball) and fundamental motor skill subscores for locomotor and object control may be attributed to population-specific characteristics. In hypermobile children, the physiological capacities assessed by these isolated fitness tests may not directly translate to competency in foundational movement patterns. This finding contrasts with existing literature in typically developing children, where muscular strength is often associated with motor competence24,25.
Locomotor and object control skills assessed in fundamental motor skill proficiency tests involve complex, multi-joint, and highly coordinated movement patterns. These skills require integration of multiple physical and neurocognitive components, including timing, spatial awareness, and rhythm, and intersegmental coordination, which are not adequately captured by isolated fitness measures. This interpretation aligns with findings by Fu et al.26, who demonstrated that functional training, rather than isolated capacity-based exercises, is more effective in improving motor performance in school-aged children. The high score on hand grip strength primarily reflects isometric force production of the forearm and hand muscles and does not correspond to the dynamic, multi-joint, sequential muscle activation required for object control skills. Similarly, the throwing a tennis ball fitness test focuses on quantitative outcomes such as speed or distance, lacking the qualitative movement criteria evaluated in TGMD-2. The flamingo balance test measures static balance and does not reflect the dynamic balance demands required for locomotor skills such as hopping or galloping, which form the foundation for more complex motor skills.
Based on these findings, it appears that coordination across multiple joints underlies fundamental motor skill proficiency. The weaker associations observed in children with generalized joint hypermobility may be related to deficits in multi-joint coordination and sensorimotor control. In children with generalized joint hypermobility, successful coordination of multiple joints, through sensory-motor integration is critical for developing fundamental motor skill proficiency. Consequently, interventions targeting impairments commonly associated with hypermobility such as joint stability, proprioception, and neuromuscular control may enhance both physical fitness outcomes and motor skill development.
4.2 Differences in the strength of association between physical fitness and fundamental motor skills according to joint mobility status
One of the key contributions of this study is the observation that the correlation coefficients between the two fitness tests (10 x 5m shuttle runs and 600m endurance run) and fundamental motor skill proficiency differed significantly between children with and without generalized joint hypermobility. Although both groups demonstrated direct associations, the strength of these relationships was markedly weaker in children with hypermobile joints.
This disparity may be attributed to biomechanical27 and neuromuscular challenges28 and commonly associated with joint hypermobility. Children with generalized joint hypermobility are more prone to joint instability, proprioceptive deficits, muscle weakness, and altered movement patterns29. Despite increased flexibility, the agility of children with hypermobility often comes at the cost of joint integrity, requiring greater muscular effort and increased reliance on visual feedback to control movement. As a result, even when physical fitness levels are adequate, motor performance may remain compromised. These findings underscore that joint-specific characteristics represent a critical variable influencing the relationship between fitness and motor coordination. Additionally, unmeasured factors such as physical activity exposure, biological maturation, and sports participation may have contributed to the observed differences in fitness and motor skill outcomes, independent of joint mobility status.
4.3 Clinical implications
Generalized joint hypermobility can negatively influence both physical fitness outcomes and fundamental motor skill development. Although proficiency in fundamental motor skills may encourage physical activity participation, it does not necessarily translate into improved physical fitness, and the reverse is also true. Therefore, targeted intervention program led by physical therapy professionals are essential for children with hypermobility. Such programs should emphasize joint stabilization, proprioceptive training, and low-impact corrective strategies to enhance physical fitness outcomes.
Interventions focusing on multi-joint movement through sensory input training may further support improvements in fundamental motor skill proficiency. In addition, parent-mediated30 intervention programs are important to reinforce professional guidance, foster a supportive home environment, and promote adherence to home exercise programs. From a physical literacy perspective, interventions for children with generalized joint hypermobility should address not only physical fitness and motor skill training but also confidence-building, enjoyment, and movement variability to support sustained long-term engagement in physical activity.
4.4 Limitations and future directions
The findings of this study should be interpreted in light of several limitations. The cross-sectional design precludes causal inference. Longitudinal studies are required to examine how the relationship between physical fitness and motor skills evolves over time and whether targeted interventions can modify outcomes in hypermobile populations. Biological maturation represents a potential confounding factor, as it differentially influences growth, body composition, and neuromuscular development in hypermobile and non-hypermobile children. The study also assessed a limited range of physical fitness components. Future research should include additional measures such as muscular strength, coordination, and dynamic balance, which may play significant roles in motor development. Psychological and behavioral factors, including motivation and habitual physical activity levels, were not assessed and may further explain variability in fitness, and motor skill outcomes. From an ICF perspective, this study focussed on Body Functions, Body Structures, and performance-based activity capacity. Participation-level outcomes and contextual factors such as environmental opportunities, psychosocial influences, and habitual physical activity were not evaluated. The absence of physical activity measurement limits interpretation of whether observed differences reflect intrinsic functional impairments or differences in activity engagement. As physical fitness may be influenced by structured sports participation, play opportunities, school-based physical education, and family support, these contextual factors should be included in future studies. Another limitation is the large number of correlation analyses conducted, which increases the risk of type I error. No formal adjustment for multiple comparisons was applied, as the analyses were exploratory. Therefore, findings should be interpreted with caution, emphasizing the consistency and magnitude of associations rather than significance of p values. Future studies should predefine primary outcomes and apply appropriate correction procedures.
4.5 Strengths of the present study
This study demonstrates several strengths, including its clear objective, robust design, and methodological rigor. By comparing correlates of physical fitness and fundamental motor skills in children with normal and hypermobile joints, the study addresses an important gap in the literature. The inclusion of a sample size larger than the estimated requirement enhances statistical power. Data were collected by trained assessors using standardized and validated assessment tools, supporting the reliability of findings. Consequently, the results are generalizable to children with generalized joint hypermobility and provide clinically relevant guidance for improving physical fitness and fundamental motor skill development.
5. Conclusion
The findings of this study indicate that joint mobility status influences the strength of the association between physical fitness and fundamental motor skills. In children with generalized joint hypermobility, mediating factors such as impaired multi-joint coordination and sensorimotor control appear to weaken this relationship. Future studies employing longitudinal designs and intervention-based approaches are needed to examine these mediators and confirm the present findings.
Acknowledgment
The authors express their sincere gratitude to Shri. Vivek Alva, Management Trustee of Alva's Education Foundation, Moodbidri, Karnataka, for his invaluable support throughout this work.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Zhang L, Wang D, Wu X. Association between fundamental movement skills and accelerometer-measured physical activity in orphan children with severe intellectual disabilities. BMC Pediatr. 2024;24:841. https://doi.org/10.1186/s12887-024-05333-6
2. Bremer E, Cairney J. Fundamental movement skills and health-related outcomes: a narrative review of longitudinal and intervention studies targeting typically developing children. Am J Lifestyle Med. 2016;12(2):148–59. https://doi.org/10.1177/1559827616640196
3. Spring KE, Carroll AV, Wadsworth DD. The relationship in early childhood body composition and physical activity levels regarding fundamental motor skill development. BMC Pediatr. 2023;23:461. https://doi.org/10.1186/s12887-023-04298-2
4. Farley JB, Stein J, Keogh JWL, Woods CT, Milne N. The relationship between physical fitness qualities and sport-specific technical skills in female team-based ball players: a systematic review. Sports Med Open. 2020;6:18. https://doi.org/10.1186/s40798-020-00245-y
5. Gao Z, Wen X, Fu Y, Lee JE, Zeng N. Motor skill competence matters in promoting physical activity and health. Biomed Res Int. 2021;2021:9786368. https://doi.org/10.1155/2021/9786368
6. Gasbarro L, Padua E, Tancredi V, Annino G, Montorsi M, Maugeri G, et al. Joint mobility protection during the developmental age among free climbing practitioners: a pilot study. J Funct Morphol Kinesiol. 2020;5(1):14. https://doi.org/10.3390/jfmk5010014
7. Chen J, Song W, Zhao X, Lou H, Luo D. The relationship between fundamental motor skills and physical fitness in preschoolers: a short-term longitudinal study. Front Psychol. 2023;14:1270888. https://doi.org/10.3389/fpsyg.2023.1270888
8. Trudelle-Jackson E, Leonard D, Morrow JR Jr. Musculoskeletal risk factors as predictors of injury in community-dwelling women. Med Sci Sports Exerc. 2014;46(9):1752–7. https://doi.org/10.1249/MSS.0000000000000295
9. Sundemo D, Senorski EH, Karlsson L, Horvath A, Juul-Kristensen B, Karlsson J, et al. Generalised joint hypermobility increases ACL injury risk and is associated with inferior outcome after ACL reconstruction: a systematic review. BMJ Open Sport Exerc Med. 2019;5(1):e000620. https://doi.org/10.1136/bmjsem-2019-000620
10. Sobhani-Eraghi A, Motalebi M, Sarreshtehdari S, Molazem-Sanandaji B, Hasanlu Z. Prevalence of joint hypermobility in children and adolescents: a systematic review and meta-analysis. J Res Med Sci. 2020;25(1):104. https://doi.org/10.4103/jrms.JRMS_983_19
11. Jari M, Alesaeidi S. Association Between Generalized Joint Hypermobility and Anxiety Disorders in Children: A Case-Control Study. Clin Med Insights Arthritis Musculoskelet Disord. 2025;18:11795441251365672. https://doi.org/10.1177/11795441251365672
12. Black WR, DiCesare CA, Wright LA, Thomas S, Pfeiffer M, Kitchen K, et al. The effects of joint hypermobility on pain and functional biomechanics in adolescents with juvenile fibromyalgia: secondary baseline analysis from a pilot randomized controlled trial. BMC Pediatr. 2023;23:557. https://doi.org/10.1186/s12887-023-04353-y
13. Ituen OA, Akwaowo CD, Ferguson G, Duysens J, Smits-Engelsman B. Impact of generalized joint hypermobility on quality of life and physical activity in school-aged children: a longitudinal study. BMC Musculoskelet Disord. 2025;26:4. https://doi.org/10.1186/s12891-024-08259-3
14. Roberts DW. Treating mechanical joint dysfunction in children: a retrospective exploratory report of selected cases. J Man Manip Ther. 2024;32(3):325–34. https://doi.org/10.1080/10669817.2022.2099182
15. de Koning L, Warnink-Kavelaars J, van Rossum M, Limmen S, Van der Looven R, Muiño-Mosquera L, et al. Physical activity and physical fitness in children with heritable connective tissue disorders. Front Pediatr. 2023;11:1057070. https://doi.org/10.3389/fped.2023.1057070
16. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–91. https://doi.org/10.3758/BF03193146
17. Smits-Engelsman B, Klerks M, Kirby A. Beighton score: a valid measure for generalized hypermobility in children. J Pediatr. 2011;158(1):119–23.e1-4. https://doi.org/10.1016/j.jpeds.2010.07.021
18. Masanovic B, Gardasevic J, Marques A, Peralta M, Demetriou Y, Sturm DJ, et al. Trends in physical fitness among school-aged children and adolescents: a systematic review. Front Pediatr. 2020;8:627529. https://doi.org/10.3389/fped.2020.627529
19. Marques A, Henriques-Neto D, Peralta M, Martins J, Gomes F, Popovic S, et al. Field-based health-related physical fitness tests in children and adolescents: a systematic review. Front Pediatr. 2021;9:640028. https://doi.org/10.3389/fped.2021.640028
20. Tun MT, Aye T, Htut TZC, Mar Tin W, Khin MT. Fundamental motor skill proficiency among 7- to 10-year-old children with Down syndrome. J Phys Ther Sci. 2023;35(1):1–6. https://doi.org/10.1589/jpts.35
21. Rey E, Carballo-Fazanes A, Varela-Casal C, Abelairas-Gómez C; ALFA-MOV Project collaborators. Reliability of the test of gross motor development: a systematic review. PLoS One. 2020;15(7):e0236070. https://doi.org/10.1371/journal.pone.0236070
22. Kavanagh H, Issartel J, Meegan S, Manninen M. Exploring the motor skill proficiency barrier among children with intellectual disabilities: analysis at a behavioural component level. PLoS One. 2023;18(11):e0288413. https://doi.org/10.1371/journal.pone.0288413
23. Bardid F, Utesch T, Stodden DF, Lenoir M. Developmental perspectives on motor competence and physical fitness in youth. Scand J Med Sci Sports. 2021;31(Suppl 1):5–7. https://doi.org/10.1111/sms.13946
24. Zhao M, Liu S, Han X, Li Z, Liu B, Chen J, et al. School-based comprehensive strength training interventions to improve muscular fitness and perceived physical competence in Chinese male adolescents. Biomed Res Int. 2022;2022:7464815. https://doi.org/10.1155/2022/7464815
25. Pitchford EA, Leung W, Webster EK. Associations of fundamental motor skill competence, isometric plank, and modified pull-ups in 5-year-old children: an observational analysis of 2012 NHANES NYFS. PLoS One. 2022;17(10):e0276842. https://doi.org/10.1371/journal.pone.0276842
26. Fu T, Zhang D, Wang W, Geng H, Lv Y, Shen R, et al. Functional training focused on motor development enhances gross motor, physical fitness, and sensory integration in 5–6-year-old healthy Chinese children. Front Pediatr. 2022;10:936799. https://doi.org/10.3389/fped.2022.936799
27. Alsiri N, Cramp M, Barnett S, Palmer S. The effects of joint hypermobility syndrome on the kinematics and kinetics of the vertical jump test. J Electromyogr Kinesiol. 2020;55:102483. https://doi.org/10.1016/j.jelekin.2020.102483
28. Tinkle BT. Symptomatic joint hypermobility. Best Pract Res Clin Rheumatol. 2020;34(3):101508. https://doi.org/10.1016/j.berh.2020.101508
29. Scheper MC, Nicholson LL, Adams RD, Tofts L, Pacey V. The natural history of children with joint hypermobility syndrome and Ehlers-Danlos hypermobility type: a longitudinal cohort study. Rheumatology (Oxford). 2017;56(12):2073-83. https://doi.org/10.1093/rheumatology/kex148
30. Wesley A, Bray P, Munns CF, Pacey V. Impact of heritable disorders of connective tissue on daily life of children: parent perspectives. J Paediatr Child Health. 2021;57(5):626-30. https://doi.org/10.1111/jpc.15284
