Original article
Intentional self-harm in Brazil: overview from 2011 to 2022 / Lesões autoprovocadas intencionalmente no Brasil: panorama de 2011 a 2022
Cíntia Mesquita Correia1 (https://orcid.org/0000-0001-5741-240X)
Larissa Silva Junquilho2 (https://orcid.org/0009-0000-6921-1904)
Paloma dos Reis Pinheiro Barbosa3 (https://orcid.org/0009-0008-4584-377X)
Gilmara Ribeiro Santos Rodrigues4 (https://orcid.org/0000-0001-7518-5757)
1Corresponding contact. Escola Bahiana de Medicina e Saúde Pública (Salvador). Bahia, Brazil. [email protected]
2,3Escola Bahiana de Medicina e Saúde Pública (Salvador). Bahia, Brazil.
4Universidade Federal da Bahia (Salvador). Bahia, Brazil.
ABSTRACT | OBJECTIVE: To analyze the sociodemographic profile of notifications of intentional self-harm in Brazil, from 2011 to 2022. METHOD: Descriptive study based on secondary data from the Information System for Notifiable Diseases (SINAN). The analysis included variables such as year, region, age group, sex, race/color, education level, and place of occurrence. RESULTS: Between 2011 and 2022, notifications of self-inflicted injuries totaled 827,659, representing a 373.5% increase (n=827,659) in Brazil, with 47.90% of cases occurring in the Southeast region, especially in São Paulo (24.17%). Adults (41.80%) and adolescents (24.41%) are the most affected, with 69.04% being women. The majority of notifications (46.60%) involve white individuals, with 16.27% having completed high school, and occurring in residences (82.43%). CONCLUSION: The data reveals a significant increase, especially among young people and women. It reinforces the need for interventions focused on vulnerable populations.
KEYWORDS: Suicide Attempt. Suicidal Ideation. Suicide. Mental Health. Epidemiology.
RESUMO | OBJETIVO: Analisar o perfil sociodemográfico das notificações por lesões autoprovocadas intencionalmente no Brasil, de 2011 a 2022. MÉTODO: Estudo descritivo a partir de dados secundários do Sistema de Informação de Agravos de Notificação (SINAN). A análise incluiu variáveis como ano, região, faixa etária, sexo, raça/cor, escolaridade e local de ocorrência. RESULTADOS: Entre 2011 e 2022, as notificações de lesões autoprovocadas totalizaram 827.659 e cresceram 373,5% (n=827.659) no Brasil, com 47,90% dos casos na região Sudeste, especialmente em São Paulo (24,17%). Adultos (41,80%) e adolescentes (24,41%) são os mais afetados, sendo 69,04% mulheres. A maioria das notificações (46,60%) envolve pessoas brancas, com 16,27% tendo ensino médio completo, ocorrendo em residências (82,43%). CONCLUSÃO: Os dados revelam um aumento expressivo das notificações, com variações por macrorregiões, faixa etária e sexo. Esses achados reforçam a necessidade de estratégias de prevenção e intervenção direcionadas às populações mais vulneráveis.
PALAVRAS-CHAVE: Tentativa de Suicídio. Ideação Suicida. Suicídio. Saúde Mental. Epidemiologia.
How to cite this article: Correia CM, Junquilho LS, Barbosa PRP, Rodrigues GRS. Intentional self-harm in Brazil: overview from 2011 to 2022. J Contemp Nurs., Salvador, 2026;15:e6262. https://doi.org/10.17267/2317-3378rec.2026.e6262
Submitted May 16, 2025, Accepted Feb. 3, 2026, Published Apr. 10, 2026
J. Contemp. Nurs., Salvador, 2026;15:e6262
https://doi.org/10.17267/2317-3378rec.2026.e6262
ISSN: 2317-3378
Assigned editors: Cátia Palmeira, Tássia Macêdo
1. Introduction
The World Health Organization defines violence as "the intentional use of physical force or power, actual or threatening, against oneself, another person, or a group or community that results in or has a high likelihood of resulting in injury, death, psychological harm, developmental disability, or deprivation"1.
Reports of violence fall into two main domains: interpersonal and self-inflicted violence. Within the scope of interpersonal violence, various forms are included, such as physical, psychological/moral violence, torture, sexual, human trafficking, financial/economic exploitation, neglect/abandonment, child labor and legal intervention. Self-inflicted violence encompasses behaviors such as suicide attempts, self-mutilation and self-flagellation2.
The suicide attempt outlines a set of deliberate behaviors aimed at inflicting harm on oneself, with the underlying intention of causing one’s own death, potentially leading to serious injury or even death. When this attempt culminates in the loss of life, it is then categorized as suicide3.
On the other hand, suicidal behavior covers a wider range of actions in which an individual expresses a predisposition to hurt or kill himself. Self-inflicted injury, a subset of this behavior, encompasses both suicidal behavior and self-aggression, which encompasses a variety of acts of self-mutilation, ranging from lighter forms such as scratches, cuts, and bites to more extreme forms such as amputation of limbs4.
Suicidal ideation, attempted suicide, and completed suicide form a complex spectrum of suicidal behavior, encompassing a range of actions related to the voluntary intention to end one’s life5. According to the International Statistical Classification of Diseases and Related Health Problems (ICD-10), self-inflicted injuries include injuries and poisonings that a person intentionally inflicts on themselves, as well as suicide attempts6.
Suicide represents a serious public health concern with continuous monitoring of mortality data related to it, carried out by the World Health Organization (WHO)7. According to information from the World Health Organization (WHO), suicide is among the top three global causes of death, being the second most common among individuals aged 15-298.
Recognized as a serious health problem on a global scale, self-inflicted injuries are closely linked to the level of individual exposure to predisposing factors. These injuries encompass a range of behaviors ranging from less severe forms such as scratches, bites and minor cuts on the skin, to more severe forms such as limb loss or even suicide. Such characteristics are fundamental and directly related to the triggering of a series of behaviors that the individual sees as a means of "escape" or temporary relief from anguish and problems. Often, these behaviors are ignored or underestimated by others, who do not recognize the importance and severity of such actions9.
Given this scenario, all forms of violence, including those self-provoked or self-inflicted, are recognized as critical events and therefore their notification is mandatory, and should be done through the Sistema de Informação de Agravos de Notificação – SINAN (Information System for Notifiable Diseases). This reporting practice is essential, as it enables governments and health services to develop targeted intervention strategies for the most-affected populations, while facilitating identification of prevalent causes in particular regions. From this information, promotion, protection and control measures can be implemented and the lack of quality in reporting records can lead to an inadequate understanding of the factors relevant for the occurrence of self-induced injuries9.
Intentional self-harm, including both suicide attempts and non-suicidal self-harm, poses a significant public health challenge worldwide. In Brazil, as well as in many other countries, these behaviors have raised growing concerns due to their devastating impact on individuals, their families and society as a whole10.
Gender, age, culture and ethnicity have important implications for the epidemiology of suicide. Between 2011 and 2022, in Brazil, the suicide rate among young people recorded an annual increase of 6%, while the rates of self-harm notifications in the 10-24 age group increased on average 29% each year in the same period. These numbers exceeded the indices of the general population, which presented an average annual growth of 3.7% in the suicide rate and 21% in the self-harm rate during this period11.
The investigation of instances of suicide attempts emerges as a crucial field of study, especially in view of the growing need for substantial data to support the formulation and implementation of strategies for improving assistance in this area. Moreover, the importance of disseminating this information in society is highlighted, aiming to foster the implementation of measures aimed at promoting mental health12. In this way, the findings are expected to contribute to a better identification and contextualization of trends about intentional self-harm.
Thus, recognizing the relevance of monitoring suicide attempts, this study presents as an objective: to analyze the sociodemographic profile of notifications for intentional self-harm in Brazil, from 2011 to 2022.
2. Method
This is a descriptive study, covering the historical series from 2011 to 2022 for intentional self-harm in Brazil. The source of data comes from Sistema de Vigilância de Violência e Acidentes/Sistema de Informação de Agravos de Notificação - VIVA/SINAN (Violence and Accidents Surveillance System/Information System for Notifiable Diseases) and collection took place in February 2024.
The notifications that were initially included in the 'interpersonal violence' record in the SINAN Individual Notification Form field were selected for analysis. After filtering, those contained in the 'self-inflicted injury' record were selected, being discriminated as 'yes' the notifications of violence and self-inflicted injuries. Notifications classified as 'interpersonal violence' were excluded. The period from 2011 to 2022 was selected because only in 2011 the notification of interpersonal/self-induced violence was included in the list of mandatory notification events.
The variables analyzed and used in this research included: year, geographical region and federative unit, age group, sex, race/color, schooling and place of occurrence. The data obtained were tabulated in spreadsheets in Microsoft® Excel software, enabling a retrospective and historical series analysis and a descriptive statistical analysis with absolute frequency values and percentages.
The study was evaluated by a Research Ethics Committee because it used secondary, non-nominal databases available for public consultation on the website of the Information and Informatics Departamento de Informação e Informática do Sistema Único de Saúde – DATASUS (Information and Informatics Department of the Brazilian Health System).
3. Results
Table 1 provides a comprehensive view of the evolution of these cases over the analyzed period, which comprises the years from 2011 to 2022. During this time interval, there was a 373.5% (n=827,659) growth in the notifications of such incidents.
There was also a gradual increase in self-harm reports from 2011 to 2019. However, in the years 2020 and 2021, during the peak of the coronavirus pandemic, there was a decrease in these notifications.
Table 1. Frequency of reported cases of self-inflicted injuries in Brazil by year, from 2011 to 2022 (n=827,659)
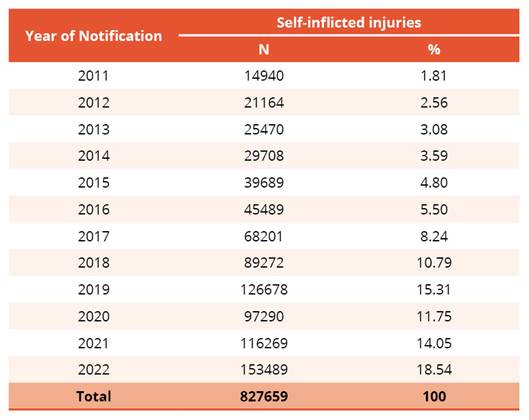
Source: Ministry of Health/SVS - Sistema de Informação de Agravos de Notificação - Sinan Net (Information System for Notifiable Diseases) (2024).
Concerning the distribution of notifications by Regions and Federative Units (FU) (Table 2), it is evident a more pronounced prevalence of reported cases of self-induced injuries in the southeastern region, totaling 47.90% of the total. Notably, the state of São Paulo stands out as an area of great concentration, representing 50.46% of the total cases reported in this region and 24.17% of the total cases reported throughout Brazil.
Table 2. Frequency of reported cases of self-inflicted injuries in Brazil by Region/Federative Unit of the Notification, from 2011 to 2022 (n=827,659)
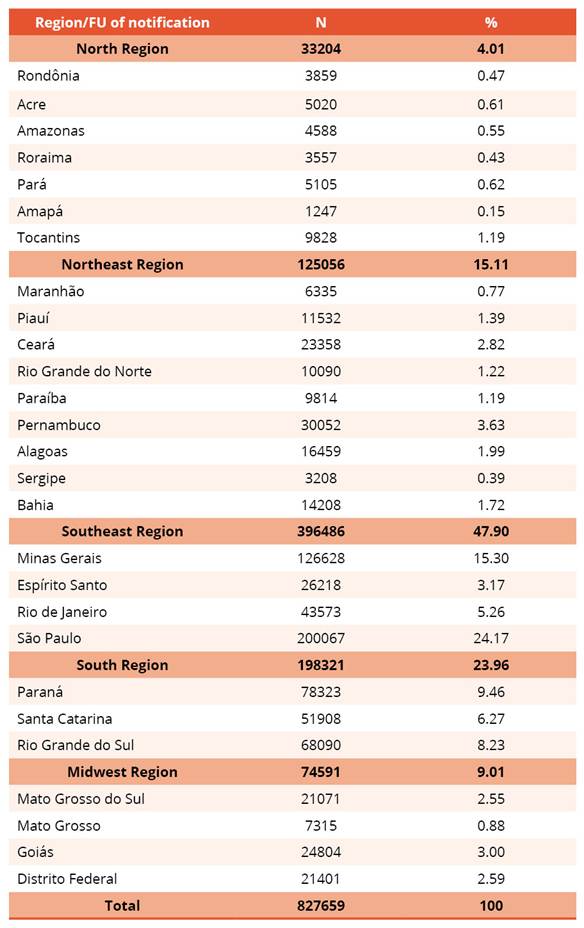
Source: Ministry of Health/SVS - Sistema de Informação de Agravos de Notificação - Sinan Net (Information System for Notifiable Diseases) (2024).
Over the period from 2011 to 2022, analyzing self-inflicted injuries reports in Brazil, it was observed predominance of the age group between 20 and 29 (28.39%), female sex (69.04%), race/color self-declared white (46.60%). Regarding schooling, 16.27% of the notifications referred to individuals whose educational background reached the level of complete secondary education. Furthermore, people with incomplete 5th to 8th grade of elementary school presented the second highest prevalence index of self-induced violence, representing 13.07% of the total in Brazil (Table 3).
Table 3. Self-inflicted injuries in Brazil according to age, sex, race/color, and education during the period from 2011 to 2022 (n=827,659)
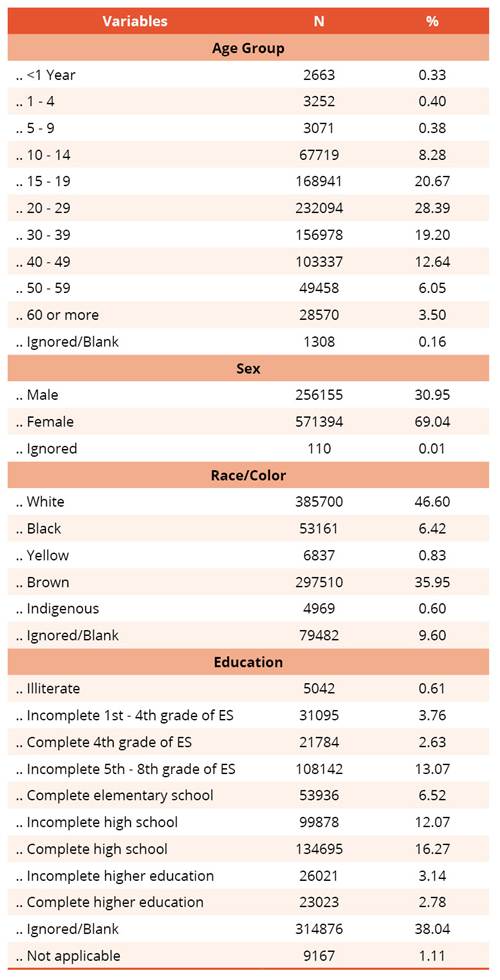
Source: Ministry of Health/SVS - Sistema de Informação de Agravos de Notificação - Sinan Net (Information System for Notifiable Diseases) (2024).
Regarding the place of occurrence, data from Table 4 show that self-inflicted injuries in Brazil during the period from 2011 to 2022 were more frequent at home (82.43%). In addition, it is relevant to consider the total of notifications at "Other", "Ignored" and "Blank" locations, which correspond to 9.88% of the total, a percentage higher than recorded for "Public streets" as the place of occurrence.
Table 4. Self-inflicted injuries in Brazil, place of occurrence, during the period from 2011 to 2022 (n=827,659)
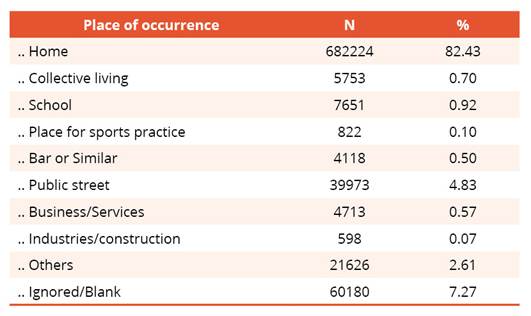
Source: Ministry of Health/SVS - Sistema de Informação de Agravos de Notificação - Sinan Net (Information System for Notifiable Diseases) (2024).
4. Discussion
The number of self-inflicted injuries reports increased significantly over the period analyzed. However, there was a temporary decrease during the years 2020 and 2021, possibly due to the COVID-19 pandemic. The drop in notifications during the pandemic period, also observed in other countries such as Japan and Australia, suggests that conditions of social isolation and difficulties in access to health services may have contributed to the underreporting of these cases. This reflects a global pattern, where public health dynamics impact the identification and recording of these behaviors13,14.
Like the study in question, several investigations have shown that at the beginning of the pandemic there was no significant increase in suicide rates. An example of this is Japan, where there was no increase in rates during the initial period of the pandemic15. Similarly, a monthly report from the Victoria state health authority in Australia found that the number of suicide deaths in September 2020 was lower than recorded in the same month 2019, indicating that, in the first seven months after the Public Health Emergency Declaration, the COVID-19 pandemic did not have a noticeable impact on suicide rates16, corroborating the findings of this study.
In Brazil, in 2012, 11,821 people died by suicide17, however, it is estimated that suicide attempts are 10 to 20 times higher than those of completed suicides18. In the Federal District, in 2019, self-inflicted injuries were the second main report, with an incidence of 21.7% for both sexes19. In the country, there were 124,709 cases of self-inflicted injuries, an increase of 39.8% compared to 201819. A study in Poland with young people aged 13 to 19 reported suicidal ideation in 24.66% of the target population, suicide plans in 15.55% and suicide attempts in 4.37% of a total of 5,685 participants20. In England, the incidence of self-mutilation increased from 174 cases (1992-1993) to 382 (2007)21. In Ireland, the rate ranged from 198 to 431 between 2002 and 2019 with a self-harm incidence rate of 206 in 2019,22 and Northern Ireland recorded 351 cases in 2019/202023.
The highest concentration of notifications occurred in the Southeast region and the state of São Paulo stood out with the largest number of notifications in the region. According to the 2022 IBGE Census24, the Southeast region is home to 84.8 million people, 41.8% of the Brazilian population, with São Paulo being the most populous state, totaling 44.4 million (21.8%). This high population density may therefore contribute to higher notification rates in the region, especially in São Paulo24.
According to a study on suicide attempts assisted by firefighters, in the state of São Paulo, there were 6,322 attempts in the pre-pandemic period (from January 2017 to February 2020), 2,296 in the pre-vaccine period of the pandemic (from March 2020 to January 2021) and 2,817 in the post-pandemic vaccination period (February 2021 to December 2021). From February 2020 to December 2021, the state of São Paulo recorded 4,456,108 COVID-19 cases. In all periods, men were more prevalent in suicide attempts25.
Within the age groups, the highest percentage of suicide attempts occurred among people aged 20-29, followed by individuals aged 15-19 and 30-39. In Eastern Europe - more specifically in the countries of Estonia, Latvia, Slovenia, Serbia, Montenegro and Hungary - the rate of suicide attempts among people aged 18 or older increased from 64 to 84 between 2012 and 201626. In China, from 2007 to 2011, 48.1% of suicide attempts in rural areas and 59.1% in urban areas occurred among people aged 15-34 years27. Thus, it can be thought that adolescents and young adults may be experiencing more frequent significant events, and that depending on the ability to cope, they may commit suicide due to severe psychological suffering.
In Brazil, between 2011 and 2017, self-inflicted injuries reported among children aged 5 to 9 years grew significantly, with 196 cases being reported28. Nevertheless, it is important to note that, despite the records, the system did not allow the attribution of self-inflicted injuries to children under 14 years old until 2014.
When compared to the international scenario, Brazil shows similarities in some respects, such as the increase of notifications in the age group 20-29 years, which is also observed in countries of Eastern Europe and in China. However, Brazil differs in presenting a higher incidence among women, who constitute 69.04% of cases, while in other contexts, men tend to be the main affected.
Another relevant data is that in the current study, self-inflicted injuries were more frequently reported among women. Studies show that although women are the most likely to attempt suicide, have a higher number of emergency services, men have the highest mortality rate, showing more success in ending their lives4,12.
Most of the notifications involved people who declared themselves white, followed by brown people. In 2019, in the Federal District, 32.35% of violence notifications were from individuals who identified themselves as brown, showing a higher incidence in this ethnic group29. However, according to authors cited above, the predominance of cases among white people does not imply that self-injury is exclusive to this group, may reflect the significant barriers faced by black populations and other racial groups in accessing health services due to structural racism. Furthermore, the study highlights the importance of a cautious analysis of these rates, since no prevalence calculation was made considering the population distribution of racial groups at the national level.
The most frequent level of schooling among reported cases was complete high school, followed by those with incomplete 5th to 8th grade of elementary education. In 2019, in the Federal District, reports of self-inflicted violence focused on individuals of both sexes with incomplete elementary school education29. In Pakistan, suicidal behavior was most common among those who had little or no schooling, with rates ranging from 30% to 60%30. It is known that in underdeveloped and developing countries where there is greater vulnerability related to socioeconomic factors, lack of adequate access to health system, education, housing, food and especially exposure to violence, the concentration of suicides is higher.
Most suicide attempts occurred in residences, with public roads being the second most frequent location. In Brazil, according to a study that evaluated the period from 2015 to 2017, 80.8% of the 78 notifications and self-inflicted injuries in children also occurred in their homes. However, 9.88% of reported cases of self-harm occurred elsewhere or was a data item that was ignored and/or left blank at the time the record was filled in28. It is thought that the home represents a more conducive environment for intentional self-harm, not only because of the availability of lethal means (medicines, cleaning products, firearms, sharp objects), as for the privacy and isolation that it provides and for being the place where the individual spends most of his time facing mental suffering.
The analyzed data suggest that a complex interaction of socioeconomic, demographic and contextual factors may influence self-harm trends in Brazil over the last decade.
The study limitations concern the grouping of data on "self-inflicted injuries" and "interpersonal violence", generating varied and contradictory results; and the possibility of underreporting or under recording of intentional self-inflicted injuries in the information system used. Moreover, the use of secondary data also involves other limitations, since data obtained from external sources do not always guarantee full reliability or accuracy and may be susceptible to failures or inaccuracies.
5. Conclusion
The analysis of notifications of intentional self-harm in Brazil, from 2011 to 2022, reveals a significant increase in cases, with a small reduction in the years 2020 and 2021, when the COVID-19 pandemic occurred, and then return of the increase. There was variation between the macroregions, with the Southeast recorded the highest number of notifications and the North region the lowest number. Regarding the sociodemographic profile, there was a predominance of female sex, young adults, white race/color and education compatible with complete high school.
The fact that the higher frequency of suicide attempts of people with lower education occurs in households evidences socioeconomic and environmental factors that can affect these behaviors. This datum reinforces the need for interventions focused on the most vulnerable populations, especially in times of crisis such as the pandemic, when isolation can exacerbate these trends.
In conclusion, despite all the limitations and the study work, the findings demonstrate the relevance of the topic as a public health problem and allow for knowledge of distribution of some variables related to suicidal behavior in the country, and the need for specific approaches adapted to each regional context.
Authors’ contributions
The authors stated that they made substantial contributions to the work in terms of research conception or design; acquisition, analysis, or interpretation of data for the work; and writing or critical review of relevant intellectual content. All authors approved the final version to be published and agreed to assume public responsibility for all aspects of the study.
Competing interests
No financial, legal or political conflicts involving third parties (government, companies and private foundations, etc.) have been declared for any aspect of the submitted work (including but not limited to grants and funding, participation in advisory board, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Contemporary Nursing is indexed in DOAJ and EBSCO.
References
1. World Health Organization. Global status report on violence prevention [Internet]. Geneva: World Health Organization; 2014. Available from: https://www.who.int/publications/i/item/9789241564793
2. Ministério da Saúde (Brazil). Viva instrutivo: notificação de violência interpessoal e autoprovocada [Internet]. 2a. ed. Brasília: Ministério da Saúde; 2016. Available from: https://bvsms.saude.gov.br/bvs/publicacoes/viva_instrutivo_violencia_interpessoal_autoprovocada_2ed.pdf
3. Conselho Regional de Psicologia do Distrito Federal. Orientações para a atuação profissional frente a situações de suicídio e automutilação [Internet]. Brasília: CRPDF; 2020. Available from: https://www.crp-01.org.br/rails/active_storage/blobs/eyJfcmFpbHMiOnsibWVzc2FnZSI6IkJBaHBBalFhIiwiZXhwIjpudWxsLCJwdXIiOiJibG9iX2lkIn19--464827fc7226855b713a4fc5bb1b48c74d25c61b/CRPDF-Orientacoes_atuacao_profissional.pdf
4. Bahia CA, Avanci JQ, Pinto LW, Minayo MCS. Self-harm throughout all life cycles: profile of victims using urgent and emergency care services in Brazilian state capitals. Cien Saude Colet. 2017;22(9):2841-50. https://doi.org/10.1590/1413-81232017229.12242017
5. Marcolan JF, Silva DA. The suicide behaviour in the Brazilian reality: epidemiological prevention policy aspects. Rev M. 2019;4(7):31-44. https://doi.org/10.9789/2525-3050.2019.v4i7.31-44
6. Organização Mundial da Saúde. CID-10 classificação estatística internacional de doenças e problemas relacionados à saúde [Internet]. 10a. rev. São Paulo: Universidade de São Paulo; 1998. Available from: https://www.edusp.com.br/livros/cid-10-1/
7. World Health Organization. Suicide in the world: global health estimates [Internet]. Geneva: World Health Organization; 2019. Available from: https://www.who.int/publications/i/item/suicide-in-the-world
8. World Health Organization. Preventing suicide: a global imperative [Internet]. Geneva: World Health Organization; 2014. Available from: https://www.who.int/publications/i/item/9789241564779
9. Almeida AA, Lima IJM, Camargo LMM, Souza RD, Oliveira WB, Santos ILF. Perfil das lesões autoprovocadas em adolescentes de 2018 a 2022 em Mato Grosso. Repositório Digital UNIVAG [Internet]. 2023. Available from: https://www.repositoriodigital.univag.com.br/index.php/enf/article/view/1882
10. Sampaio TCSM, Lima CH. Systematic review on self-injury in Brazil and in the world. Res Soc Dev. 2022;11(9). https://doi.org/10.33448/rsd-v11i9.30731
11. Sebastião M. Estudo aponta que taxas de suicídio e autolesões aumentam no Brasil [Internet]. Rio de Janeiro: Fiocruz; 2024. Available from: https://portal.fiocruz.br/noticia/2024/02/estudo-aponta-que-taxas-de-suicidio-e-autolesoes-aumentam-no-brasil
12. Nacamura PAB, Salci MA, Paiano M, Pini JS, Melo WA, Jaques AE, et al. Mortality from self-infringement: trend analysis. Enferm Foco. 2022;13:e-20227. https://dx.doi.org/10.21675/2357-707X.2022.v13.e-20227
13. Santos IN, Silva BVP, Carlomanho AMF, Morais CS, Pernambuco ML. Social isolation and its impacts on mental health: A review. Res Soc Dev. 2021;10(8):e22110817206. https://doi.org/10.33448/rsd-v10i8.17206
14. Organização Pan-Americana de Saúde. Considerações para o ajuste de medidas sociais e de saúde pública no contexto da COVID-19 [Internet]. Washington: OPAS; 2020. Available from: https://iris.paho.org/bitstream/handle/10665.2/52179/OPASWBRACOVID1920065_por.pdf?sequence=1
15. Isumi A, Doi S, Yamaoka Y, Takahashi K, Fujiwara T. Do suicide rates in children and adolescents change during school closure in Japan? The acute effect of the first wave of COVID-19 pandemic on child and adolescent mental health. Child Abuse Negl. 2020;110. https://doi.org/10.1016/j.chiabu.2020.104680
16. Leske S, Kõlves K, Crompton D, Arensman E, Leo D. Real-time suicide mortality data from police reports in Queensland, Australia, during the COVID-19 pandemic: an interrupted time-series analysis. Lancet Psychiatry. 2021;8(1):58-63. https://doi.org/10.1016/S2215-0366(20)30435-1
17. Silva BFA, Prates AAP, Cardoso AA, Castro NGMBR. Suicide in contemporary Brazil. Soc Estado. 2018;33(2):565-79. https://doi.org/10.1590/s0102-699220183302014
18. Peixoto E, Palma B, Farias I, Zanini D, Santana N, Bueno J. Questionário de impulsividade, autoagressão e ideação suicida para adolescentes (qiais-a): propriedades psicométricas. Psicol Saúde Doenças [Internet]. 2019;20(2):271-85. Available from: https://scielo.pt/pdf/psd/v20n2/v20n2a01.pdf
19. Secretaria de Saúde do Distrito Federal (Brazil). Informe epidemiológico anual de violência interpessoal e autoprovocada no Distrito Federal, 2019 [Internet]. Brasília: Secretaria de Saúde; 2020. Available from: https://www.saude.df.gov.br/documents/37101/822596/INFORME-EPIDEMIOLOGICO-2019-2020-corrigida-2.pdf
20. Zygo M, Pawłowska B, Potembska E, Dreher P, Kapka-Skrzypczak L. Prevalence and selected risk factors of suicidal ideation, suicidal tendencies and suicide attempts in young people aged 13–19 years. Ann Agric Environ Med. 2019;26(2):329-36. https://doi.org/10.26444/aaem/93817
21. Bergen H, Hawton K, Waters K, Cooper J, Kapur N. Epidemiology and trends in non-fatal self-harm in three centres in England: 2000-2007. Br J Psychiatry. 2010;197(6):493-8. https://doi.org/10.1192/bjp.bp.110.077651
22. Joyce M, Daly C, Mcternan N, Griffin E, Nicholson S, Arensman E, et al. National self-harm registry Ireland annual report 2019 [Internet]. Cork: National Suicide Research Foundation; 2020. Available from: https://www.nsrf.ie/wp-content/uploads/2021/04/NSRF-National-Self-Harm-Registry-Ireland-annual-report-2019-Final-for-website.pdf
23. Public Health Agency. Northern Ireland registry of self-harm - summary regional report - 2019/20 [Internet]. Belfast: Public Health Agency; 2022. Available from: https://www.publichealth.hscni.net/publications/northern-ireland-registry-self-harm-annual-report-2018-2019-and-summary-report-2019
24. Instituto Brasileiro de Geografia e Estatística. De 2010 a 2022, população brasileira cresce 6,5% e chega a 203,1 milhões [Internet]. Rio de Janeiro: IBGE; 2023. Available from: https://agenciadenoticias.ibge.gov.br/agencia-noticias/2012-agencia-de-noticias/noticias/37237-de-2010-a-2022-populacao-brasileira-cresce-6-5-e-chega-a-203-1-milhoes
25. Wagner GA, Almeida TRF, Araújo AL, Munhoz DM, Andrade PG. Time series analysis of the suicide attempts assisted by firefighters from 2017 to 2021 in São Paulo, Brazil. Rev Bras Epidemiol. 2022;25:e220026. https://doi.org/10.1590/1980-549720220026
26. Stevovic LI, Vodopic S. Attempted suicide in Podgorica, Montenegro: higher rates in females and unemployed males. Ann Gen Psychiatry. 2017;16(1):15. https://doi.org/10.1186/s12991-017-0151-5
27. Li L, Liu C, Tong Y, Wu J, Zhou W, Yin Y, et al. Comparison of characteristics of suicide attempts registered in urban and rural areas in China. Front Psychiatry. 2022;12. https://doi.org/10.3389/fpsyt.2021.805324
28. Avanci JQ, Pinto LW, Assis SG. Notifications, hospitalizations and deaths from self-harm in children in Brazil’s national health systems. Cien Saude Colet. 2021;26(suppl 3):4895-4908. https://doi.org/10.1590/1413-812320212611.3.35202019
29. Silva NN, Favacho VBC, Boska GA, Andrade EC, Merces NP, Oliveira MAF. Access of the black population to health services: integrative review. Rev Bras Enferm. 2020;73(4). https://doi.org/10.1590/0034-7167-2018-0834
30. Shekhani SS, Perveen S, Hashmi DS, Akbar K, Bachani S, Khan MM. Suicide and deliberate self-harm in Pakistan: a scoping review. BMC Psychiatry. 2018;18(1):44. https://doi.org/10.1186/s12888-017-1586-6
